Specsavers has officially been named the 4th Best Workplace in Australia by Great Place To Work® – a testament to our vibrant, inclusive, and people-first culture.
This recognition reflects our ongoing commitment to delivering exceptional hearing care while creating a workplace where everyone feels valued, supported, and inspired to grow. Join a team that’s setting the standard – in hearing care and in culture. Explore careers at audiology-anz.com.au
IT’S ON: REGULATION FOR AUDIOLOGISTS BUT AUDIOMETRISTS MISS OUT
In one of Australia’s biggest hearing health developments, audiologists will be regulated after the nation’s health ministers confirmed they would amend law to regulate the profession.
Peak audiology, audiometry and consumer bodies welcomed the decision which the Department of Health, Disability and Ageing confirmed was anticipated to take a minimum of at least two years to implement based on previous experience and the time required to make legislative amendments.
Inclusion of audiology will see the establishment of mandatory national registration, protection of title for audiologists, and a complaints process under the Australian Health Practitioner Regulation Agency (Ahpra).
But the only body that represents audiometrists and audiologists, the Australian College of Audiology
incorporating HAASA (ACAud inc. HAASA), said audiometrists were excluded which was “surprising and concerning”.
Dr Sonj Hall, CEO of ACAud inc. HAASA, said it had advocated for audiometrists' inclusion. The Audiology Decision RIS and the Independent review of complexity in the NRAS – developed to support the decision-making process – had also recommended including audiometrists, she said.
“We were formally advised by the National Health Secretariat that under the Health Practitioner Regulation National Law, audiometrists will not be included in the scope of national regulation for audiology,” Dr Hall said. “While we welcome the national regulation of audiologists, we are disappointed that audiometrists have been excluded.
“We are deeply concerned
for our audiometrist members, who make up a significant portion of Australia's hearing health workforce. Many are understandably worried – not only for the future of their profession, but for the communities they serve, particularly in areas where access to hearing care is already limited.
"We will continue to fight for inclusion and recognition.”
ACAUD INC. HAASA WANTS AUDIOMETRIST RECOGNITION FOR MEDICARE ITEMS
ACAud inc. HAASA has lodged its formal submission to the MBS Review Advisory Committee advocating for audiometrists to be recognised as eligible providers under seven audiology and allied health Medicare items.
The Australian College of Audiology incorporating the Hearing Aid Audiology Society of Australia (ACAud inc. HAASA) said this was “a vital step to improving access to affordable hearing care, especially in regional and rural Australia”.
CEO Dr Sonj Hall said nearly 70% of audiometrists already served in regional and rural areas (MMM 2–6), yet they were not fully recognised within the MBS.
“Our submission to government calls for audiometrists to be
included in select Medicare items, so more Australians can get timely, affordable hearing care – without unnecessary travel or delays,” she said.
“We are advocating for recognition of audiometrists as eligible providers for a defined set of MBS audiology and allied health items, to improve access to hearing care especially in regional, rural and First Nations communities.”
The organisation is seeking recognition on the following assessment items which can currently be performed by eligible audiologists with a GP referral:
• 82306 - Non determinate audiometry
• 82309 – Air conduction
• 82312 - Air and bone
conduction audiogram or air conduction and speech discrimination audiogram
• 82315 - Air and bone conduction and speech discrimination audiogram
The Health Ministers Meeting in Perth on 12 September 2025 confirmed audiology would be regulated under the National Registration and Accreditation Scheme (NRAS). Audiologists will join 16 other health professions regulated under Ahpra which administers NRAS.
A communique said: “Health Ministers noted the updated Audiology Decision Regulatory Impact Statement which affirmed the option of regulating the audiology professions under the NRAS. Health Ministers agreed to amend the Health Practitioner Regulation National Law, following further policy work, to regulate the audiology profession under the NRAS structure.”
The Health Workforce Taskforce will lead the transition which will require further policy work and amendments to the law, a
continued page 8
• 82318 - Air and bone conduction and speech discrimination audiogram with other cochlear tests
• 82324 - Impedance audiogram involving tympanometry and measurement of static compliance and acoustic reflex
• 81310 - Aboriginal or Torres Strait Islander Australians who have had a health assessment.
Dr Hall said fitting and services outside Medicare would continue as per existing practice and employer/clinical policies.
continued page 8
Helping hands for ears in Fiji
A volunteer trip by Australian audiologist mates Sandra Lee and Sachinthya Dona has had a positive impact on hearing services in Fiji including upskilling staff, supporting a hospital ear health department launch and adapting the Kendall Toy Test to a local language.
Above: Leanne Emerson (top left, clockwise), Dr Sonj Hall, Rae Walker and Rachael Gibson. Images: AudA, ACAud inc. HAASA, IAA, Deafness Forum Australia.
Image: Sandra Lee.
NEWPLATFORM NEWCHIP
THE DIFFERENCE IS CLEAR
Widex presents the new Widex Allure powered by the W1 chip with Precision Hearing Technology and Widex Compass Cloud, the world’s first cloud-based fitting software. This combination of new and advanced features aims to balance crystal clear speech with accurate environmental sound, delivering natural sound quality.
IN THIS ISSUE
18 The disability gap Audiologist Dani Fox appeals to hearing practitioners to help close the intellectual disability gap.
20 A clearer view Ear visualisation equipment is a vital tool of the trade for hearing practitioners. Check out advances and trends.
EDITORIAL
TURN IT DOWN FELLAS!
As the mother of twin sons, I am used to loud noise. Things were marginally quieter with just our daughter but once the boys arrived, noise levels increased abruptly and have continued that path. We encouraged their outdoor passions and sports, resisting pleas for X-boxes, PlayStations, and iPads. When they began secondary school, they received mobile phones and finally, when they turned 14, we gave in and bought a PlayStation.
Loud gaming is one thing I worry about when it comes to their hearing. I often hear extremely loud gaming noise coming from their rooms. I ask if they would like to be wearing hearing aids in a few years, and mention that if they don’t turn it down, that may be the case. This warning works for a bit and the volume reduces but inevitably the loudness returns.
26 A successful model Specsavers Audiology has conducted 4.3 million hearing screenings since arriving in Australia.
28 Widex's W1 chip Widex has launched its new W1 chip in Australia, debuting in innovative Allure hearing aids.
Getting the message across to young people isn’t easy but the World Health Organization has been trying to do that by introducing safe listening standards and resources. It warns that one billion young people are putting their hearing at risk by listening to excessively loud music, whether at events or through earbuds or headphones, as well as noisy gaming.
I reckon ads showing inner ear hair cells dying when blasted with loud music/gaming shown on streaming services, TikTok, TV, radio, during gaming, and at school might be a start.
One innovative initiative which kicked off this year – HELA or Healthy Ears, Limited Annoyance – is a step in the right direction and helps venues implement a global standard for safe listening at music events. It provides affordable, accessible online certification for staff who work at venues and events. You can read more about this in HPA’s feature with one of HELA’s founders, Dr Jos Mulder from the Australian National University, on page 16. If the message can cut through to my sons – and their generation – then perhaps we will see a future where young people don’t just hear the music and games they love, but still hear clearly for decades to come.
HELEN CARTER Editor
Image: Dani Fox.
Image: Alison Chiam.
Image: Widex.
Image: Specsavers.
Australia’s Leading Manufacturer of Hearing testing rooms
Our hearing testing rooms are designed in house, with expert knowledge, made from premium materials and individualised to your specific needs.
Product Offering
• Micro booth relocatable solution for testing in industrial and medical situations. Commonly used for work screenings and pre-employment scans.
• Modular Micro Booth Modular booths are demountable, making them easily adaptable to fit through smaller, unique spaces. These units are brilliant for testing
• Test Lab person booth with increased noise attenuation, creates an environment to give more data for an audiologist or an ENT specialist.
• Large Testing Room customisable rooms aimed to achieve the lowest possible ambient noise level to be used in paediatrics, bone conduction testing, or VROA.
Contact us to assist you in selecting the room that will suit your clients needs.
E. admin@adfi.com.au
P. 03 9775-0340
adfindustries.com.au
UPFRONT
Just as HPA went to print, the FEDERAL GOVERNMENT announced that more than 260,000 children nationwide each year would have stronger protection against pneumococcal disease with a new and improved vaccine. Prevenar 20 is now available through the National Immunisation Program. Pneumococcal disease is a bacterial infection caused by Streptococcus pneumoniae which can cause pneumonia, bloodstream infection, meningitis and ear infections, specifically otitis media. It replaces Prevenar
OFF THE BEATEN TRACK
Weird
Griffith University researchers have developed a publicly available tool to help scientists uncover what’s going on beneath the surface of rivers, using sound. The tool makes it easier to track changes in biodiversity and discover new species. It was developed in R, a free program for analysing data where users upload a folder of audio files and sort through vast volumes of audio. The tool scanned recordings and detected sections from Warrill Creek, Kalbar that contained sound, grouping similar sounds together.
Wonderful
Expression Australia has teamed up with Disney and Birde – child-friendly audio speakers – to bring Disney stories to life in Auslan.
13 and Pneumovax 23. IN OTHER NEWS, therapeutics scientist and molecular biologist, Professor Sue Fletcher AO, has been appointed senior honorary research fellow at Ear Science Institute Australia. She is internationally esteemed for her work in genetic and molecular research, which has fuelled advancements in molecular therapies for hereditary diseases such as Duchenne muscular dystrophy and retinitis pigmentosa. The collaboration will see her leverage her expertise to partner with Ear Science’s multidisciplinary teams, particularly Hearing Therapeutics to improve ear and hearing health outcomes. Research projects will target genetic and
STAT
molecular mechanisms underlying ear diseases and hearing loss. They also aim to accelerate development of diagnostics and devices for ear and hearing disorders and elevate application of laboratory discoveries into therapeutic interventions such as gene therapies. FINALLY, Hearing Practitioner Australia is proud to adopt an inclusive font this edition to use going forward. The font, specifically designed to be easier for those with low vision to read, is Atkinson Hyperlegible, developed by the Braille Institute. This typeface features clear and distinctive letterforms to improve legibility and readability. The font is free to download and use via Google Fonts and the Braille Institute.
Expression Australia said the collaboration had created five tap and play books with complimentary Auslan signing videos. The child taps on the speaker, and the story comes alive on a smart TV with a presenter signing the story in Auslan. Expression Australia said Birde was easy for children to use on their own.
Wacky
Scientists have found day-active moths have larger hearing organs than their nocturnal relatives, despite facing less threat from echolocating bats. Researchers set out to test whether diurnal moths have reduced tympanal organs which allow them to detect high frequency calls that bats use to locate prey at night. They expected reduction or loss of hearing organs in the diurnal species but the opposite was true, suggesting their enlarged ears detected lower-frequency sounds produced by birds or reptiles.
Milestone 5,000 cochlear implants performed
The Royal Victorian Eye and Ear Hospital celebrated with the recipient Mrs Margaret Pearce (above far right) who was implanted at age 95. Page 39.
WHAT'S ON
THIS MONTH AUDIOLOGY AUSTRALIA ONLINE CONFERENCE
23 & 24 OCTOBER
Australian audiology's premier home conference is back. Eight hours of education and CPD will be delivered across two half days. audiology.eventsair.com/audaonline25
Complete calendar page 51
NEXT MONTH 2025 DEAFBLINDNESS CONFERENCE
27 & 28 NOVEMBER
The Sydney conference brings together individuals and families with Dual Sensory Impairment – Deafblindness and professionals. Dsiproject.org.
Publisher Sarah Baker sarah.baker@primecreative.com.au
The spokesperson said the Hearing Services Program (HSP) requires all clinicians who deliver services under it to be a member of a Practitioner Professional Body (PPB). But HSP Qualified Practitioner requirements would be amended, as required, to remain consistent with broader regulatory settings while supporting program and client objectives.
Peak audiology body, Audiology Australia (AudA), said the decision for audiology regulation had been broadly supported by AudA members and was a significant step towards strengthening the profession’s reputation.
“Reflecting decades of advocacy from Audiology Australia, registration under NRAS will deliver important outcomes, including title protection, stronger safeguards for the public, and consistent standards across public and private sectors,” AudA CEO Ms Leanne Emerson said.
“This is a fantastic development in our ongoing efforts to heightened recognition of the important role that audiologists play to treat Australians with hearing and balance concerns and to safeguard the Australian public.”
AudA recognised the hard work of members and others in the sector who provided feedback on consultations and advocated for the profession.
Emerson said it was unclear how the decision would be implemented but possible broader reforms to the scheme may run concurrently with work to bring audiology into NRAS.
“Further detail will be available on our website as it comes to hand,” she said. “AudA is committed to a smooth transition and will work closely with government and policymakers to ensure the model delivers outcomes that audiologists and the community expect.”
Independent Audiologists Australia (IAA) said the move was “a landmark achievement for public safety, professional accountability, and the future of hearing healthcare”. President Ms Rachel Gibson said it was the result of more than a decade of sustained advocacy by IAA for “stronger, nationally consistent regulation".
“This is a win for every Australian who relies on high-quality, ethical, and evidence-based audiological care,” she said, adding that IAA had “long argued that audiology must be regulated like other allied health professions to ensure public protection”.
IAA commended health ministers and the department for progressing “this long-overdue reform” and welcomed the chance to contribute to policy and legislative work.
“As the Australian professional body representing independent audiologists, IAA looks forward to working closely with governments to
“IT'S A LANDMARK DECISION FOR AUDIOLOGY AS A PROFESSION.”
DR
DAYSETAVORA-VIEIRA, AUDIOLOGIST
ensure the new regulatory framework is fit-for-purpose, protects consumers, and recognises the unique value of independent practice,” Gibson said. It stressed the importance of clearly defining the scope of the new regulation and ensuring standards reflected qualifications, expertise, and ethical obligations of audiologists
Deafness Forum Australia said after many years of lobbying the move was “a historic milestone for Australian hearing health”. “As the national voice for hearing health consumers, Deafness Forum Australia welcomes this decision as a win for Australians with hearing loss,” chair Ms Rae Walker said.
“Aligning audiology services with the governance, complaints, and disciplinary structures applied to other allied health professions will only benefit those requiring hearing health services. Making audiologists subject to independent oversight will provide greater public trust and increased consumer confidence when seeking audiology services."
Perth audiologist Dr Dayse Távora-Vieira said it was “a landmark decision for audiology as a profession” and marked the formal recognition of audiology’s vital role in healthcare.
“Ahpra registration protects the public by ensuring practitioners are properly qualified, competent and accountable, and fosters greater trust in the delivery of hearing health services,” she said.
MOVE WOULD CLOSE GAP, GIVING MEDICARE REBATES
continued from page 3
“The (requested) change is who Medicare recognises, not a change to clinical scope,” she said. “It is well within an audiometrist’s recognised scope of practice to assess, fit, program and verify hearing devices independently with no audiologist supervision required.
“Today, billing eligibility for the listed MBS items is limited to eligible audiologists. This does not reflect clinical practice, where audiometrists work independently in public and private settings often side-by-side with audiologists.”
She said that clinically, audiometrists already performed these assessments independently across Australia but under Medicare, only an eligible audiologist could bill these items on medical practitioner referral.
“That means consumers can
receive a Medicare rebate – and be bulk-billed where offered – only when the service is provided by an eligible audiologist,” Dr Hall said.
“If the same assessment is performed by an audiometrist, no Medicare rebate is currently available. This is one of the gaps our submission seeks to close.”
She said the items were especially important for improving hearing care in communities that were harder to reach, such as those in rural and regional Australia.
“Audiometrists play a crucial role in supporting access for Aboriginal and Torres Strait Islander communities, who often face additional barriers to hearing services,” she said. “Providing cost-effective audiology services helps eliminate financial barriers for patients seeking hearing healthcare, while offering greater choice and cultural fit.”
Recognising the items would also help unlock under-utilised workforce capacity, supporting a more sustainable hearing healthcare system that could meet growing patient demand, Dr Hall added.
“Most importantly, it would contribute to closing critical gaps in hearing care, delivering more equitable outcomes across the country,” she said. It would immediately help overcome shortages of audiologists in rural and remote areas. “It would help now and start to prepare us for rising demand,” Dr Hall said. “Enabling audiometrists to bill the assessment items would relieve current shortages outside major centres and, as more Australians engage earlier with their hearing, we’ll need more qualified clinicians overall.
“This approach complements – not replaces – audiologists and supports a sustainable pipeline to meet growing community need.”
Image: Dayse Távora-Vieira.
Dr Sonj Hall, ACAud inc. HAASA CEO. Image: ACAud inc. HAASA.
DEMENTIA OUR LEADING CAUSE OF DEATH
Dementia is now the leading cause of death for Australians, according to a new Australian Institute of Health and Welfare report which also states untreated hearing loss is a risk factor that increases the likelihood of developing dementia.
The AIHW’s updated web report Dementia in Australia was released on 12 September 2025. It found that in 2023, there were 17,409 deaths due to dementia, making it the leading cause of death overall. The second leading cause was coronary heart disease which caused 16,922 deaths.
Dementia was the main cause of death in women, killing 10,890 and causing 12.5% of deaths among women. It was the second leading cause of death in men, killing 6,519 and causing 6.8% of all deaths in men, after coronary heart disease (10,343).
Almost one in ten deaths were from dementia and the report warned that without significant intervention, the number of Australians living with the condition would exceed one million by 2065, up from 425,000 in 2024.
Professor Tanya Buchanan, Dementia Australia CEO, said the report, released in the lead-up to
Dementia Action Week, revealed the enormous impact dementia has on Australian families.
“These figures highlight just how many families are impacted by dementia across Australia. Most of us know someone who is or has been impacted by dementia,” she said. “It is more pressing than ever that the federal government commit to funding a national conversation on dementia to raise awareness and promote brain health at all ages.”
The report referred to the 2024 Lancet Commission on dementia prevention, intervention, and care which found hearing impairment was equal top of the list of modifiable risk factors associated with the greatest proportion of people developing dementia globally.
dementia include obesity, smoking, excessive alcohol consumption, air pollution, head injury, high blood pressure, untreated hearing loss, untreated vision loss, depression and diabetes.
“Protective factors that reduce the likelihood of developing dementia include high levels of education, physical activity, social engagement and cognitive activity (such as through education or cognitively stimulating work).
“People who engage in protective factors and avoid risk factors are less likely to develop dementia and tend to develop dementia at older ages.”
The Lancet report estimated the risk factors associated with the greatest proportion of people developing dementia were hearing impairment and high LDL (low-density lipoprotein) or “bad” cholesterol in midlife; each was responsible for 7% of dementia cases globally.
Drawing on this, the AIHW report said: “Risk factors that increase the likelihood of developing
YOUNGER HEARING
AID
The report also said the World Health Organization had developed recommendations on the types of interventions that should be adopted to reduce risks associated with cognitive decline and dementia and these included managing hearing loss.
It said 43% of the dementia burden in Australia could be attributed to six modifiable risk factors: being overweight or obese, physical inactivity, high blood sugar, high blood pressure in midlife, smoking and impaired kidney function.
WEARERS HAVE 61% LOWER RISK OF DEMENTIA: ANALYSIS
A new analysis of the Framingham Heart Study suggests hearing aid wearers under age 70 have a reduced risk of developing dementia compared with people the same age with hearing loss who do not use hearing aids.
The American researchers said their finding highlighted the importance of early intervention for hearing loss for possible prevention of dementia. “To our knowledge, this observational study was the first to identify that reduced risk depends on early intervention for HL (hearing loss),” they said.
They said participants with hearing loss and hearing aids showed reduced risk for dementia among those younger than 70 at the time of hearing evaluation, when followed for up to 20 years.
“Compared with participants with HL without hearing aids, participants with HL with hearing aids had a 61% lower risk for incident all-cause dementia among
those younger than 70 years at HL diagnosis; participants with no HL had a 29% lower risk for incident all-cause dementia,” they said. This risk was unaffected by additionally adjusting for either Framingham Stroke Risk Profile or educational level.
But they found no association between hearing aid use and incident dementia in people 70 years or older.
Neurology professor Dr Sudha
It was the first to identify reduced risk depends on early intervention. Image: Zinkevych/ stock.adobe.com.
Seshadri and colleagues reported findings in a research letter in JAMA Neurology on 18 August 2025. They said age-related HL was a known risk factor for developing dementia.
They examined prospectively whether self-reported hearing aid use by people with HL was associated with lower risk of incident dementia in the Framingham Heart Study original and offspring cohorts and explored interactions with age.
Among 2,953 participants (mean age 68.9 and 59% who were female) followed for up to two decades, 583 (20%) developed incident all-cause dementia. Of these people, 245 (42%) were younger than 70 at hearing assessment.
“Other studies, including a randomised clinical trial and a comprehensive meta-analysis, have suggested that hearing aids have a protective benefit against development of dementia,” they wrote.
Participants self-reported their hearing aid use.
Prof Tanya Buchanan, Dementia Australia CEO. Image: Dementia Australia.
IN BRIEF
BALLOON DILATION
The American Academy of Otolaryngology–Head and Neck Surgery has released a position statement on paediatric Eustachian tube balloon dilation (ETBD), stating it is appropriate, efficacious and safe in a select group of children. The statement said the academy considers the procedure as an “appropriate treatment for paediatric patients with obstructive Eustachian tube dysfunction resulting in chronic otitis media which is refractory to standard surgical interventions such as tympanostomy tube placement and adenoidectomy”. “Multiple studies have demonstrated the efficacy and safety of ETBD in the paediatric population, with evidence showing improvements in hearing, tympanogram, quality of life, and decreased likelihood for additional surgery,” it stated. It said the procedure could be completed safely as a stand-alone procedure or in combination with other procedures.
PRAC PAYMENT
Allied Health Professions Australia (AHPA) has called for the Commonwealth Prac Payment (CPP) to include all health professions to help tackle placement poverty during clinical placements. AHPA, whose members include Audiology Australia, wrote to Mr Jason Clare, the Minister for Education, seeking a commitment to an immediate expansion of the CPP to include all allied health professions. AHPA also requested a meeting to discuss the path forward for broadening the program. Allied health students and leaders including Ms Bronwyn Morris-Donovan, AHPA CEO, put their case to politicians at Parliament House on 28 July 2025. The payment was announced in the 2024-2024 Federal Budget and started on 1 July 2025 for nursing, midwifery, teaching and social work students.
SPRITZ-OM GRANT
A Western Australian research program which is developing a nasal probiotic therapy called Spritz-OM to prevent childhood ear infections has received a $300,000 grant to progress the project. The therapy aims to use ‘friendly’ bacteria to guard the ear from otitis media (OM) and reduce overuse of antibiotics. CUREator, a national biotechnology incubator, announced new top up funding will develop assays to enable phase one patient sample analysis and the generation of clinical proof-of-concept data for phase two trials. The research program is based at The Kids Research Institute Australia in Perth.
ONE IN THREE KEEP HEARING LOSS A SECRET
One in three adults aged over 50 are keeping their hearing loss a secret, often because they fear being judged, new research shows.
The large-scale international research program found hearing loss is still linked to stereotypes about ageing and disability, which can stop people from seeking help.
The June 2025 special issue of the International Journal of Audiology featured eight research papers that explored how stigma affects adults with hearing loss, their families, and the professionals who support them.
The research involved interviews, surveys, and real-world video recordings with adults who have hearing loss, their partners, and hearing care professionals. It also included an online survey of more than 600 people across Australia, the US, and the UK.
Researchers said one of the most striking findings was the difference in perspective between people with hearing loss and the professionals who treat them. While clinicians focused on the stigma of hearing aids, adults were more concerned about the stigma of hearing loss itself. In fact, many patients described modern hearing aids as discreet, high-tech, and helpful.
Those who talked openly about their hearing loss were more likely to accept and use hearing aids. But for many, that first conversation was the hardest part.
hearing loss said others had laughed at or joked about their hearing difficulties, leaving them feeling uncomfortable and frustrated. Many chose to hide their hearing loss, which could make things worse.
Dr Ekberg said understanding how people feel about hearing loss was key to improving care. “The more we know, the better we can support people to feel confident, seek help, and communicate openly,” she said.
Dr Ekberg said asking questions such as, “Who do you tell about your hearing loss?” can help professionals understand emotional barriers their clients face.
“For adults with hearing loss, telling others can be a helpful step in working through stigma, though it may require support from professionals and loved ones,” she said.
“For families and the broader community, raising awareness about acquired hearing loss –which often begins from age 50 – can help challenge outdated stereotypes that associate hearing loss only with very old age.”
The research team developed practical resources to support adults with hearing loss, hearing care professionals, families, and the public. These include infographics that can be displayed in clinics or used as conversation starters with clients and other health professionals.
Study co-lead Dr Katie Ekberg from Flinders University. Image: Flinders University.
Led by Dr Katie Ekberg from Flinders University and Professor Louise Hickson AM from The University of Queensland, the research highlighted the emotional and social toll of hearing loss and why it’s time to talk about it.
Nearly 60% of people with
Dr Ekberg and Prof Hickson edited the journal's special issue which addressed gaps in research by providing a more comprehensive understanding of the stigmatising experiences of adults with acquired hearing loss and their families in relation to hearing loss and use of amplification.
Other researchers involved in the project were Dr Barbra Timmer, Professor Nerina Scarinci, Dr Mansoureh Nickbakht and Dr Monique Waite from the University of Queensland, and Dr Carly Meyer from Bolton Clarke.
The researchers said about 3.6 million Australians live with hearing loss and it wasn't just about missing sounds but could lead to low self-esteem, loneliness, memory problems, and depression.
The Hearing Industry Research Consortium funded the project.
TGA APPROVES LENIRE TONGUE STIMULATION DEVICE FOR TINNITUS TREATMENT IN AUSTRALIA
The Therapeutic Goods Administration (TGA) has approved Neuromod Devices’ Lenire tongue stimulation device for use by tinnitus patients in Australia, with audiologists and ENT surgeons likely to have major roles in its prescription and management.
A TGA spokesperson told HPA it had approved the Lenire tinnitus therapy auditory/translingual electrical stimulation system on 11 September 2025 and listed it as a medical device included class 11a on the Australian Register of Therapeutic Goods.
The listing states: “Lenire device is intended to be used by tinnitus sufferers of at least 18 years of age to alleviate the symptoms of chronic, subjective tinnitus. It should be used for 30 to 60 minutes per day, every day, for at least 10 weeks, after which you may experience sustained alleviation of your tinnitus symptoms.
“The Lenire device can be used in the home environment after
qualified healthcare professional.” It said the device was intended for prescription use only as use by a person for whom the device had not been configured may cause discomfort, or temporary exacerbation of tinnitus loudness.
In a media release on 23 September 2025, Neuromod Devices, the medical technology company that created Lenire, said: “Patients with tinnitus are prescribed Lenire by an appropriately qualified healthcare professional, such as an audiologist or ENT surgeon, after an assessment for suitability and can complete treatment from home in between follow-up appointments with their clinician.”
The device delivers mild pulses to the tongue. Image: Eoin Holland for Neuromod Devices.
tongue via 32 electrodes on a proprietary device trademarked as Tonguetip. Settings can be configured to provide treatment with different combinations of audio and electrical stimuli. Timing, intensity and delivery of stimuli are controlled by a handheld controller that each participant is trained to use before continuing treatment from home.
Neuromod announced Lenire had European Medical Device Single Audit Program (MDSAP) approval and EU Medical Device Regulation (MDR) certification.
Bimodal neuromodulation is stimulation of nerves with two paired stimuli for therapeutic purposes. Lenire consists of wireless (Bluetooth) headphones that deliver sequences of audio tones to both ears, combined with electrical stimulation pulses delivered to the surface of the
Dr Ross O'Neill, Neuromod founder and CEO, said: "MDSAP and MDR certification allow Neuromod to continue expanding Lenire's availability in Europe while positioning the company to commercialise Lenire in new geographies such as Australia, Canada and beyond."
Neuromod said Lenire was the first non-invasive bimodal neuromodulation tinnitus treatment device shown to soothe and relieve tinnitus in clinical trials.
Muffled sounds and painful ear infections are a thing of the past for 100 Aboriginal children who have received free life-changing grommet surgery through Western Australia’s Djaalinj Waakinj research program.
The program, which launched in 2018, recently celebrated the milestone 100th surgery performed by paediatric ear, nose and throat surgeon Associate Professor George Sim at St John of God Murdoch Hospital. He has consulted with more than 350 children through the program over the past seven years.
The procedures were made possible through a partnership between the hospital, A/Prof Sim, the Wesfarmers Centre of Vaccines and Infectious Diseases, based at The Kids Research Institute Australia, and Cockburn Integrated Health.
Djaalinj Waakinj, which means listening and talking in Noongar language, connects ear health researchers with Aboriginal and Torres Strait Islander families in Perth’s south metropolitan area. The research program conducted by the Wesfarmers Centre is based at The Kids Research Institute Australia.
Researchers visit babies from two months of age to check for early signs of otitis media (OM) and hearing loss. They said about 50% of Aboriginal children suffer debilitating OM by six to eight months but the program has been life changing for more than 430 families who accessed free, fast-tracked urgent specialist treatment and grommet surgery.
Associate Professor Val Swift, co-director for the Djaalinj Waakinj centre, and Aboriginal cultural guidance advisor at the Wesfarmers Centre, said the ability to avoid a long waitlist for treatment had an immeasurable impact on these children.
“OM can cause permanent hearing loss if not caught and treated early, but unfortunately, many children are living with untreated ear disease over a long period of time, which causes long-term issues with language, behavioural and educational development,” she said on the Kids Research Institute Australia website.
Staff from the hospital helped fund the surgeries by raising more than $140,000. Combined with contributions from St John of God Health Care, this took the total raised to just under $220,000.
Surgeon A/Prof George Sim with Jahkye Harris and his mum Nikki Naylor. Image: The Kids Research Institute Australia.
SPECSAVERS NAMED FOURTH BEST WORKPLACE
Great Place to Work has recognised Specsavers as one of Australia’s Best Workplaces for 2025, ranking it fourth in the top 10 of the large business category.
This marks the third consecutive year Specsavers has earned a place on the list. Specsavers said it was a standout achievement that reflected its strong workplace culture and leadership in the retail hearing care sector.
This year’s assessment of confidential employee feedback was also the largest evaluation of workplace culture in Australia’s history, capturing insights from 158,749 employees across all sectors and organisation sizes.
As a business committed to transforming hearing health across Australia, this recognition reinforced the connection between a thriving workplace and exceptional clinical care, Specsavers said.
“This recognition is a reflection of the culture we’ve built – one that empowers audiology professionals to deliver the highest standard of care,”
Australia's private hospitals do more than half of the nation's ENT surgery. Image: Jixiang/stock. adobe.com.
said Mr Tom Craw, managing director – audiology at Specsavers ANZ.
“When our people feel supported and inspired, it directly impacts the quality of service and outcomes for our customers. A great workplace culture enables us to deliver great hearing care.”
With a growing network of audiology professionals in more than 320 stores nationwide, Specsavers was making hearing care more accessible, affordable, and customer-focused, he said.
Specsavers’ said its people-first approach was embedded in every part of its audiology business. workplace culture in Australia’s history.
PRIVATE HOSPITALS ASSOCIATION WANTS MORE PUBLIC PATIENTS
“This would reduce pressure on public hospitals, improve patient outcomes, and see spare capacity in private hospitals optimised.
The Australian Private Hospitals Association (APHA) has called for state and federal governments to partner with private hospitals for positive productivity.
Speaking before the Treasurer’s Economic Forum in August 2025, APHA reminded decision-makers of the vital contribution private hospitals make to the health economy and that it needs to grow.
APHA said most ENT surgery in Australia was done in private hospitals. In 2023-2024, 53% of ear, nose and throat diseases treatment was performed in private hospitals.
“We need a funding model that fosters public patients in private hospitals more consistently, supported by long-term commitments rather than ad hoc
“Aligning these reforms under the National Health Reform Agreement with private hospital capabilities will support more sustainable federal and state budgets, ease government capital expenditure on public facilities and better promote innovation.”
Heffernan said APHA remained positive about the role of private hospitals in Australian healthcare delivery, but it needed federal and state governments to “come with us” and “it doesn’t have to cost anything”.
“Taxpayers get a massive return on zero investment in private hospitals. Just 633 private hospitals carry out 70% of planned surgery, 61% of acute mental healthcare, 81% of rehabilitation and 1.66 million medical treatments each year, including 54% of chemotherapy,” he said.
More than 5.14 million patients were admitted to private hospitals last year, up 3% on the year before.
Image: Great Place to Work.
HBA PERTH SEMINAR HIGHLIGHTED TRENDS AND CHALLENGES IN HEARING SERVICES
Trends and challenges in hearing services, along with sustainable business models, were the main focus of Hearing Business Alliance’s Perth seminar.
The seminar, at Perth Mercure on 23 July 2025, brought together business owners, audiologists, audiometrists and key stakeholders from across the hearing sector.
Ms Jane MacDonald, HBA’s CEO, said 24 delegates attended from 20 independent audiology businesses and 11 exhibitors supported the event, with 18 trade delegates attending.
Starkey was the major sponsor.
“The seminar focused on current trends and emerging challenges in hearing services, with sessions covering regulatory changes, workforce issues, and the future of hearing technology,” she said.
“Attendees heard from industry leaders, legal and financial experts, and government representatives, gaining insights into best practices and innovations shaping the sector.”
MacDonald said a strong theme throughout the day was the need for sustainable business models in the face of evolving client expectations and policy reforms, plus improved client clinical outcomes.
Presentations also addressed
Services Program (HSP), strategies for managing business risk, and approaches to attract and retain skilled staff.
“The seminar provided a valuable opportunity for networking and peer learning and reinforced the importance of collaborative approaches to ensure the long-term viability and impact of hearing service providers,” she said.
“Feedback from delegates was extremely positive.”
MacDonald spoke about key HBA activities, strategic insights and gave a small business update.
Speakers and topics included:
• Mr Stephen Logan, HBA business manager, who gave the opening address on unlocking knowledge.
• Dr Pádraig Kitterick, head of audiological science at the National Acoustic Laboratories, who discussed NAL-NL3, the next generation hearing aid fitting system.
• NSW audiometrist Mr Daniel Fechner and Queensland audiologist Mr Christo Fourie who introduced AudZone, Australia's first AI-powered platform for hearing care professionals and clinics.
• Mr Fechner, director and audiometrist from Ear Studio, also spoke about the value of data modern CRM (customer relationship management) systems for business management.
• Ms Gabby Luksza, acting assistant secretary, Hearing Services Branch, Department of Health, Disability and Ageing, spoke about proposed HSP changes, expanding on members’ questions.
• Ms Belinda McLean, general manager of HR Focus, discussed navigating employment laws including key Australian legislation, compliance essentials, and avoiding legal pitfalls. HR Focus works with small and medium sized businesses who require advice and assistance with HR and workplace safety.
• Mr Steven Le, consumer support specialist and trainer with Starkey, gave the major sponsor update on pushing the edge of possibility with Edge AI. Delegates gained six endorsed CEP points for ACAud inc HAASA and AudA in category 1.1.
LEADERSHIP CHANGES AT WS AUDIOLOGY ANZ AND APAC
WS Audiology has announced changes in its leadership for Australia and New Zealand, as well as Asia Pacific.
WSA managing director of wholesale and retail ANZ, Mr James Benston, has been promoted to president of WSA’s APAC region. Benston, who started his career nearly 30 years ago in Brisbane as a technician building hearing aids, began his new role on 1 October 2025.
He joined the company’s executive committee on that date, the hearing healthcare group announced in a media release. Benston succeeds Mr Olivier Chupin, who WSA said had decided to leave the company after four successful years to pursue a career outside WSA.
Audiologists Ms Rebecca Gay and Mr Grant Ewer are now leading WSA in Australia and New Zealand (ANZ).
WSA announced that Gay had been appointed to lead its wholesale business in ANZ, while Ewer would take on responsibility for the retail business. Their appointments began on 1 October 2025, the company
announced in another media release.
WSA said Gay and Ewer were experienced leaders with long-standing ties to the hearing care industry and to WSA. They would work closely together to drive growth, and to support partners across Australia and New Zealand.
WSA promoted Gay to managing director of Wholesale ANZ, and said her appointment marked a significant step in its investment in leadership excellence and commitment to delivering value to wholesale customers.
With more than two decades of experience in the hearing care industry, Gay bring a unique blend of clinical expertise and strategic acumen to the role, WSA said. Since joining the company in 2009, she had held several senior positions including most recently commercial director of Wholesale ANZ where she played a pivotal role in driving commercial performance and strengthening customer relationships.
She has a Master of Clinical
Promotions for Grant Ewer (from left), Rebecca Gay and James Benston. Images: WSA.
psychology from the University of Sydney. Gay will report to Benston and join the APAC leadership team.
Mr Jan Makela, CEO of WSA, said he was thrilled to welcome Benston to the executive committee and as the new APAC president. “He is an experienced and strong leader with a unique understanding of the hearing aid industry and its people,” Makela said.
“He began his career at WSA nearly three decades ago as a technician building hearing aids in the Brisbane office. Since then, he has steadily advanced through the ranks and most recently led our successful Australian and New Zealand markets.”
Image: Hearing Business Alliance.
CHARLES DARWIN UNIVERSITY’S AUDIOLOGY ENROLMENTS SKYROCKET
Enrolments in the Charles Darwin University’s (CDU) Master of Clinical Audiology have increased by more than 500% since the program launched in 2022, the university has revealed.
The university is primarily based in the Northern Territory. It said the number of enrolled audiology students had grown from the equivalent of four full-time students in 2022 to more than 24 in 2024, demonstrating strong demand for the only online audiology degree in Australia.
CDU said the surge reflected its growing role in addressing critical gaps in hearing health services, particularly in the Northern Territory, which has the highest rates of hearing loss and ear disease in the country – disproportionately affecting First Nations communities.
Mx Mich Thornton, CDU senior lecturer in audiology (Faculty of Health), said the program was developed specifically to meet pressing workforce needs in urban and remote settings. “There’s an
urgent need for more audiologists across Australia, and especially in the Territory,” Thornton said.
First-year CDU audiology student, Ms Holly Rasmussen, a qualified speech pathologist, said the need for more audiologists was clear in her day-to-day work. “You can’t help children learn to speak if they can’t hear you,” she said. “There is a real and urgent need for more hearing health professionals in regional and remote areas.”
Meanwhile, patient appointments delivered by audiology students at CDU’s Health Hub have nearly tripled in under three years.
Professor Nicole O’Reilly, CDU Head of School, Allied Health Sciences said CDU audiology students provided 91 appointments in 2023, 186 appointments in 2024, and 251 appointments in 2025.
The Health Hub is CDU’s multidisciplinary training and community clinic, where students in health disciplines provide supervised care to the public while gaining hands-on clinical experience in fields
Speech pathologist and CDU audiology student Holly Rasmussen from Nevertire in rural NSW. Image: CDU.
including audiology, psychology and occupational therapy.
Much of the care is delivered free of charge to people who may otherwise have no access to essential services, with students providing care under the supervision of clinical educators.
“CDU launched its expanded Health Hub (formerly Wellness Centre) in 2024 as the Faculty of Health broadened its student-led clinic offerings,” Prof O’Reilly said.
Overall, the Health Hub has more than doubled its service delivery over the past two years, with client numbers, student placements and partnerships recording significant growth, she added.
Since 2023, client demand had increased by 120%. Student placements had also surged, including in audiology. Overall, they rose from just over 1,100 days in 2023 to more than 3,000 in 2025 –a 165% increase.
Federal Government funding enabled expansion of clinical placements and service offerings.
MAMMALIAN COCHLEA KEPT ALIVE OUTSIDE THE BODY
FOR THE FIRST TIME
American researchers have kept a tiny cochlea sliver from a gerbil alive and functional outside of the body for the first time and watched it work in real time as they played it sounds from a speaker.
The Rockefeller University scientists designed a chamber which imitated the living environment of the cochlea and placed a sliver of cochlea tissue inside.
They said the cochlea’s fragility and inaccessibility embedded in the densest bone in the body generally made it difficult to study in action.
They excised gerbil cochlea slivers no larger than 0.5 mm in the region that picks up the middle range of frequencies.
They timed the excision to a developmental moment in which the gerbil’s hearing was mature, but the cochlea had not fully fused to the temporal bone.
They then played sounds via a tiny speaker to the cochlea.
The researchers said they witnessed the opening and closing of ion channels in hair bundles (protruding from hair cells) add energy to sound-driven vibrations,
amplifying them. They also saw how outer hair cells elongated and contracted in response to voltage changes through electromotility.
“We could see in fine detail what every piece of the tissue was doing at the subcellular level,” said postdoctoral fellow Dr Francesco Gianoli on The Rockefeller University news website.
“We can now observe the first steps of the hearing process in a controlled way that was previously impossible.”
The chamber reproduces the living environment of the sensory tissue, including continuously bathing it in nutrient-rich liquids called endolymph and perilymph and maintaining its native temperature and voltage.
Above: Dr Jim Hudspeth with zebrafish which he used to study hearing. Image: Mario Morgado/ The Rockefeller University.
The device allowed the scientists to capture live biomechanics of the rodent cochlea’s auditory powers, including exceptional sensitivity, sharp frequency tuning, and the ability to encode a broad range of sound intensities.
Dr Gianoli is co-author of two studies in PNAS and Hearing Research which described the
“remarkable advancement” achieved by neuroscientist Dr A. James ‘Jim’ Hudspeth and his team at the university’s Laboratory of Sensory Neuroscience.
Dr Hudspeth had been working on this for more than 20 years, said Rockefeller biophysicist Professor Marcelo Magnasco who described it as “a crowning achievement for a remarkable career”.
Dr Hudspeth and his team achieved the breakthrough shortly before his death in August 2025. The university said the innovation was a product of his five decades of work illuminating molecular and neural mechanisms of hearing.
Join leaders from Australia and around the world for 8 hours of online learning across broad areas of audiology to suit your
1. Watch live 23-24 October
2. Watch on-demand 27 October – 19 January
3. Watch some sessions live, then the rest on demand REGISTER NOW
https://audiology.eventsair.com/ audaonline25
A HELAva good time without damaging hearing
A groundbreaking initiative to help venues implement a global standard for safe listening at music events launched this year. HELA (Healthy Ears Limited Annoyance) provides short online certification for those working in the live music and dance industries.
Alarmed at unsafe listening practices at music events, senior lecturer at the Australian National University’s School of Music, Dr Johannes (Jos) Mulder and colleagues overseas have created an initiative that aims to reduce the risk of damaging hearing.
For many years, some argued that music was less harmful because it was not industrial noise, he says, but “now we know that loud music can be as harmful to ears as a machine”.
A former sound engineer, Dr Mulder transitioned 15 years ago to academia where, apart from teaching, his research focuses on the dangers of entertainment sound, particularly loud music at concerts, and the risk of hearing damage from headphone listening and video gaming.
“We know that entertainment sound is often too loud. People go dancing and are exposed to dangerously loud sound, go to concerts and knowingly expose themselves and come home with big threshold shifts, beeping in their ears and all sorts of issues,” he says.
Studies show this exposure can lead to hearing loss and tinnitus.
In 2018, Dr Mulder began collaborating with four colleagues from the Audio Engineering Society (AES), a global body for audio engineers, the industry and research. They came up with the idea of music industry certification to reduce hearing damage from exposure.
“We thought, if you want to be a chef or work in a restaurant, you need to have demonstrated skills to ensure you don't place your customers at risk of food poisoning, whereas anyone can rock up to venues and crank up the music,” he says.
“That has to change because you need people who, in addition to technological skills and communication skills, also understand what they’re doing in terms of sound and the risk they're bringing to audiences, musicians and workers.”
The group expanded to 10 including audiologists, sound engineers and communication experts. They surveyed more than 2,500 sound engineers in 63 countries and found most would undertake safe listening certification and be willing to attend training to gain certification.
They presented their idea for education and certification at the International Conference on Audio Education online in July 2021 during the COVID pandemic.
The group spent two years devising a curriculum for online safe listening certification for event staff, venue owners and patrons.
“Halfway through, we realised we shouldn’t just be targeting audio engineers or the person at the mixing desk but also venue management, the people who do the security and pick up the empty glasses, door staff and patrons,
as all are exposed,” Dr Mulder says.
“Called Healthy Ears, Limited Annoyance or HELA, the certification is like food hygiene training but for your ears.”
While initially aimed at training venue staff on sound safety, it has evolved to be for all key stakeholders in the live event industry.
“This groundbreaking initiative aims to set a new global standard for safe listening at live events by educating venue staff, managers and others on safe listening practices and certifying them worldwide to implement WHO (World Health Organization) safe listening standards,” Dr Mulder says.
LOW COST ENABLES ACCESSIBILITY
The creators split training into a simple core version for general awareness to educate event staff on how to protect their ears and reduce risks at concerts and venues, and a more advanced version for audio engineers and technical managers.
It includes best practice and covers audience expectations, acoustic and sound system design, hearing health, management and communication.
Security staff at nightclubs are also exposed to loud music.
HELA helps venues implement safer listening at music events. The HELA certified badge (below left).
The cost of $10 per person for the core 45-minute course, and $30 for the half day advanced course, makes it accessible to all and provides certification for five years, Dr Mulder adds. A quiz must be passed afterwards to gain certification.
All revenue goes to research with the HELA Research Co-op, which launched in August 2025, allocating funds to projects. It will receive funding from UK Research and Innovation, which funds research in the UK, for three years to get started while slowly building revenue from the HELA certificates.
Training is not positioned as occupational health and safety (OHS) training. Dr Mulder says sound would have to be 80-83 decibels over eight hours to qualify under OHS regulations, depending on the region, – much lower than any music venue. Also, fans could only attend a typical pub gig or rock venue for 7.5 minutes if it was an OHS rule at this level.
When the organisers finished the course design in 2024, they approached industry including manufacturers of loudspeakers. They were happy to support the initiative and help fund it to get off the ground through Derby University in the UK.
The NightTime Industries Association (NTIA) also came on board. A peak UK body that represents nightclubs, cafes, bars and venues, it already had a hearing preservation campaign, Listen for Life with partners including Specsavers Audiology. But it made HELA a partner also and included it in its campaign.
“HELA launched on World Hearing Day in 2025 and everyone who works in these venues is invited to take the certificate. When all staff are certified, a venue can say it is certified,” Dr Mulder says.
“Certification is open to the world. We’re working with a peak European body for music venues which represents about 3000 venues. Brazil and South America are very interested, and we’ll create a Spanish version soon.”
There are ongoing trials and collaborations globally with stakeholders, audiologists, audio engineers, music and hospitality bodies.
In Australia, Dr Mulder’s first year students at ANU have completed certification and will be surveyed to determine if it’s suitable to include in courses for music, dancing and audio engineer students.
HELPS IMPLEMENT WHO STANDARD
Importantly, HELA certification is a support mechanism to help venues, workers and staff implement the WHO Global standard for safe listening venues and events, released in 2022.
Dr Mulder is a member of the consultation group for the WHO’s Make Listening Safe initiative, created in 2015, which aims to make recreational listening safe. The initiative developed the venues standard,
“HELA certification is like food hygiene training but for your ears. It’s a support mechanism to help (music) venues and staff implement WHO safe listening standards.”
and another, the Global standard for safe listening devices and systems.
The venues standard states 1.1 billion young people are at risk of hearing loss because of unsafe listening practices and 40% of people aged 12 to 35 in high and middle income countries are exposed to damaging sound levels in entertainment venues.
Dr Mulder says HELA is based on work carried out by the Audio Engineering Society (AES) Technical Committee on Acoustics and Sound Reinforcement and the WHO’s Make Listening Safe Initiative, specifically the WHO’s Technical Working Group on the Global standard for safe listening venues and events.
From 2018 to 2020 an AES working group on sound exposure and noise pollution due to outdoor entertainment events critically analysed the problem. It worked on sound level monitoring at live events including regulations, practices and preferences, tools and procedures.
“The venues standard puts the maximum limit at 100dB, A-weighted, equivalent loudness measured over 15 minutes at music events. This is still dangerously loud, so you still need hearing protection, but it aims to stop ‘stupid loud’,” he says. “It’s had a lot of buy-in from governments, venues, health bodies, and hearing bodies.”
The standard comprises six features which, when implemented, allow audience members to enjoy amplified music while protecting their hearing, and preserving integrity of the artistic experience.
The features allow a maximum limit of 100 decibels over 15 minutes, to facilitate a compromise between safe and enjoyable.
Dr Jos
Mulder ANU
They also ensure safe listening through live monitoring and recording of sound levels by staff using calibrated equipment, and optimisation of venue acoustics and sound systems.
The standard specifies personal hearing protection such as earplugs and designated quiet zones should be available for audience members, and audience members and staff should be informed of practical steps to ensure safe listening.
The course information says audiences expect venues and events to be operated responsibly and a commitment to professionalism is central to meeting this expectation. Non-technical staff including bar staff, security and door staff, venue managers and owners also have a responsibility towards safe listening, the HELA website states.
Dr Mulder’s next step is getting Australia on board, engaging Australian stakeholders and promoting the initiative further here.
He recommends reusable ear plugs for music events, which can be bought for about $20, but he says they’re worth it. The message is people can still have a ‘HELAva good time’ at music events without damaging their hearing, he adds.
The HELA website sums it up nicely.
“HELA isn't just about turning down the sound levels or putting earplugs in your ears – it's about smart sound management that benefits audiences, artists, and communities alike; education presented in a digestible way and learning how to prevent your hearing from being destroyed while doing something you love.”
Learn more at helainitiative.com.
Audio technicians are prone to hearing loss due to their prolonged exposure to loud music.
Image: killykoon/stock.adobe.com.
Image: Dr Jos Mulder.
Closing the disability gap
The Disability Royal Commission revealed a 27-year difference in life expectancy for Australians with intellectual disability. Audiologist DANI FOX reveals how hearing practitioners can help.
for people with intellectual disabilities by providing them better access to healthcare.
She is passionate about the cause, and not just because she is the parent of a child with Down syndrome, but because she sees widespread discrimination and knows hearing practitioners are compassionate people who can make a difference.
Fox has twin daughters, aged 12; ‘Miss Zee’ (not her real name) has Down syndrome and wears bilateral hearing aids while ‘Miss Cee’ is neurotypical.
The Royal Commission into Violence, Abuse, Neglect and Exploitation of People with Disability began in 2019 and handed down its final report in 2023.
At the Audiology Australia 2025 Conference in Adelaide, Fox told Zee’s story and asked delegates to join her in tackling failures in the health system that the commission found contribute to the large gap in life expectancy for people with intellectual disability (ID).
“The Disability Royal Commission found there was a 27-year gap in life expectancy due to systemic failures in the health system, historically and that is continuing today; 27 years,” Fox said. “I just want to pause and let that soak in.”
Zee’s life expectancy is nearly three decades less than her sister’s, she stressed.
“Hearing health, and hearing health professionals, are such an important part of this bigger picture,” she said. “We are supporting people like Zee to hear better, so they can learn better, communicate
better, participate in society better.
“As a profession, we are not just integral to the wellbeing of people with ID, we are foundational to the wellbeing of a person with ID, which ripples out across the whole lifespan. What we do in our day-to-day job makes a difference!”
Zee has physical disabilities, ID and bilateral fluctuating conductive hearing loss. “She has had seven grommet surgeries and spent about half of her life experiencing life through at least one glue ear,” Fox said.
She also has auditory processing disorder and myopia (requiring glasses), hypotonia (meaning her muscles have low tone), and hypermobility which makes her joints flexible and unstable, impacting her mobility. Additionally, she has auditory and visual sensory sensitivities so can become overwhelmed in complex auditory or visual environments, similar to what autistic people commonly experience.
Intellectually, Zee has cognitive issues, learning and language development delays, speech difficulty and working memory problems.
“Zee is a person with an intellectual disability but firstly, she is a person, who happens to have an ID,” Fox said.
The Royal Commission’s final report: Our Vision for an Inclusive Australia and Recommendations, documented health care experiences for people with ID. Fox said it showed that Zee was more likely to: • be refused health care than her sister • not seek healthcare services than her sister
• not be spoken to in her appointments, have her opinion sought or her experience heard
• not have a say in her healthcare treatment plans or what happens to her
• not be able to understand information provided to her in appointments because it’s provided for higher health literacy levels or as auditory information only
• not go back to her healthcare provider because the environment is not inclusive, makes her anxious, has too many barriers or overtly excludes her – “we don’t see people with ID here”.
The Royal Commission’s vision for the future is for people with disabilities to be safe, have their human rights respected, have disability treated as part of human diversity and live, learn, work, play, create and engage in inclusive communities.
“It wants people with ID to be empowered to have choices and independence, belong and be respected, valued and able to contribute, and be culturally safe,” Fox said, adding there are clear Equal Opportunity laws and an Australian National Road Map for healthcare for people with disability.
IN THE CLINIC
In the clinic setting, “it’s our collective and shared responsibility”, Fox said. “All organisations and private businesses should take on these recommendations including hearing health organisations and clinics.”
Following the Royal Commission, a Council for Intellectual Disability (CID) was established to support health professionals,
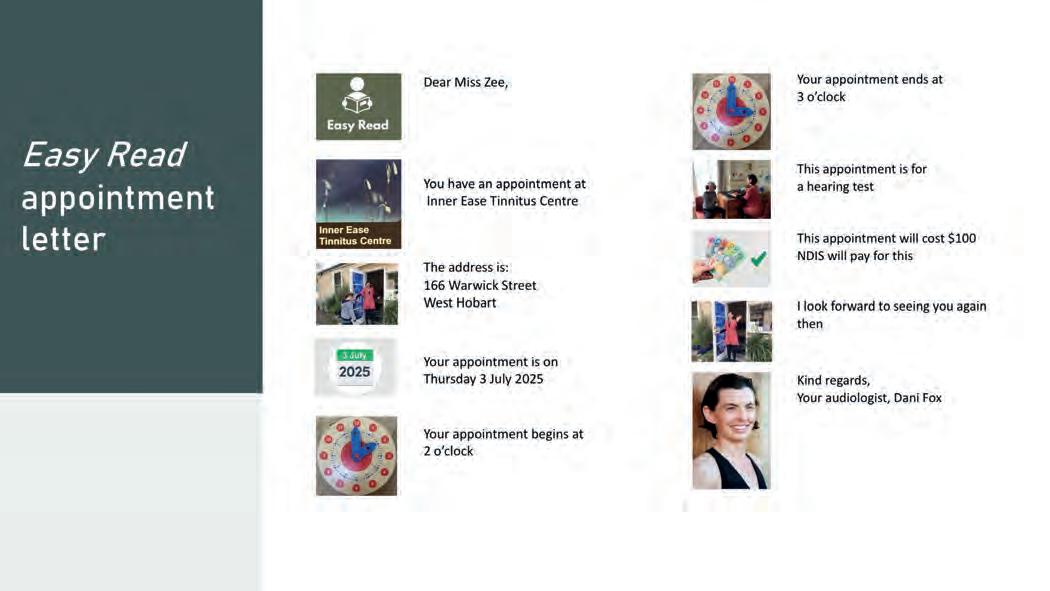
An example of an “easy read” appointment letter.
Images: Dani Fox.
‘Miss Zee’.
Fox showed a video at the conference of Down syndrome health ambassador Ms Naomi Lake saying people with ID were encouraged and supported to participate in their community. Segregation in health, education, and sport, etc was in the past.
“People with intellectual disability want their voice to be heard, they want to be seen,” Lake said. “They want lifelong education, important work, social engagement. This all leads to better health outcomes across the lifespan.”
Fox said clients with ID had progressive views and expected their hearing health practitioner to include them.
TIPS TO PROMOTE INCLUSION
The Convention of Rights of Persons with Disability says “substantive equality” appreciates that some people may need different treatment to achieve equitable outcomes and protect their human rights. This can be achieved through “reasonable adjustments” as recommended by the Royal Commission and the Council for Intellectual Disability, Fox said.
“You have a real opportunity to make a huge difference in their lives. Because they experience so much inequity in the system, this is your chance to make it right.”
Dani Fox Inner Ease Tinnitus Centre
The commission and the council urged these adjustments in all healthcare settings to promote inclusion and achieve better health outcomes, and whole life well-being.
Fox said practitioners could make reasonable adjustments by introducing measures she has implemented in her clinic including:
• Preparing for the visit by sending an “easy read” appointment letter before each visit.
• Ensuring the waiting room is a calm space, or a quiet space can be offered.
• O ffering a break during long appointments, and as needed, and including a break card for the client to hand over.
• Using a visual schedule on a board. This can have drawings on sticky notes that are removed as tasks happen which enables clients to know what’s happening next and gives a sense of timing.
• Adding a timer.
• Allowing the client to have input on the consultation schedule such as the order and what is included or excluded on the day.
• Using a whiteboard schedule.
• Supporting communication and rapport with conversation cards that talk about clients’ health. The cards are freely available to print from the CID website (cidc.org.au) or practitioners can make their own clinic specific ones.
• Supporting understanding and two-way communication with augmented assistive communication visuals which are an adjunct to spoken language throughout the appointment.
• Provide information in “easy read” format.
• Provide clear next steps in written/visual format; write it, text it, email it, photograph it. Ask the person with intellectual disability their preference.
The Council for Intellectual Disability
(cidc.org.au) makes resources to improve communication between people with intellectual disability and health workers. It can design “easy read” information, conversation cards, and folders where people keep their health information, to improve communication between people with an ID, supporters and health workers.
Fox said feeling anxious, unsafe or afraid might be expressed as behaviour such as stimming (repetitive behaviours such as rocking, tapping, vocalising or chewing on items), unexpected actions, being distracted or hyperactive.
“Reasonable adjustments in place will minimise feelings of anxiety, and help people feel calm,” she said. “Implementing these tools helps establish a feeling of safety for the person coming to the appointment, and a way of connecting and establishing a rapport with the clinic staff and clinician.”
Calmer behaviours allow people to be more open and receptive to learn – and take on therapy, Fox added. “When a person feels safe, their behaviours will be calm and relaxed, open to engaging with you, they’re able to access more words and language to communicate with you, are open to taking in information and learning, and open and receptive to treatment and rehab recommendations; in other words, they’ll have better health outcomes.”
Conversely, negative behaviours are most often the way a person with ID communicates if feeling stressed, anxious and unsafe. “What else can you do to help your client feel safe, calm and relaxed? If unsure, ask them; they will know what makes them feel safe and calm,” she said.
“Consider what you can do differently, rather than expecting the person with ID
to do the adjusting which has historically led to poor health outcomes and gap in life expectancy.”
The commission found that what people with intellectual disability want in health consultations is for practitioners to:
• Speak clearly and slowly.
• Talk directly to the client, not the support worker.
• Allow time to answer questions.
• Write things down. Show visuals.
• Provide “easy read” information.
• Give clear next steps.
• B e patient. Don’t rush. Provide breaks. Take more time.
“As hearing health professionals, this is especially important because when people have their hearing and communication needs met, they're less likely to experience abuse and neglect, and more able to reach their full potential, participate and contribute meaningfully to society, and live a full, rich and long life,” Fox said.
“When a person with intellectual disability seeks your help for their hearing health care, you have a real opportunity to make a huge difference in their lives. Because they experience so much inequity in the system, this is your chance to make it right.”
Dani Fox presenting at the Audiology Australia 2025 Conference in Adelaide.
Sisterly love, ‘Miss Cee’ and ‘Miss Zee’.
Image: Prime Creative Media.
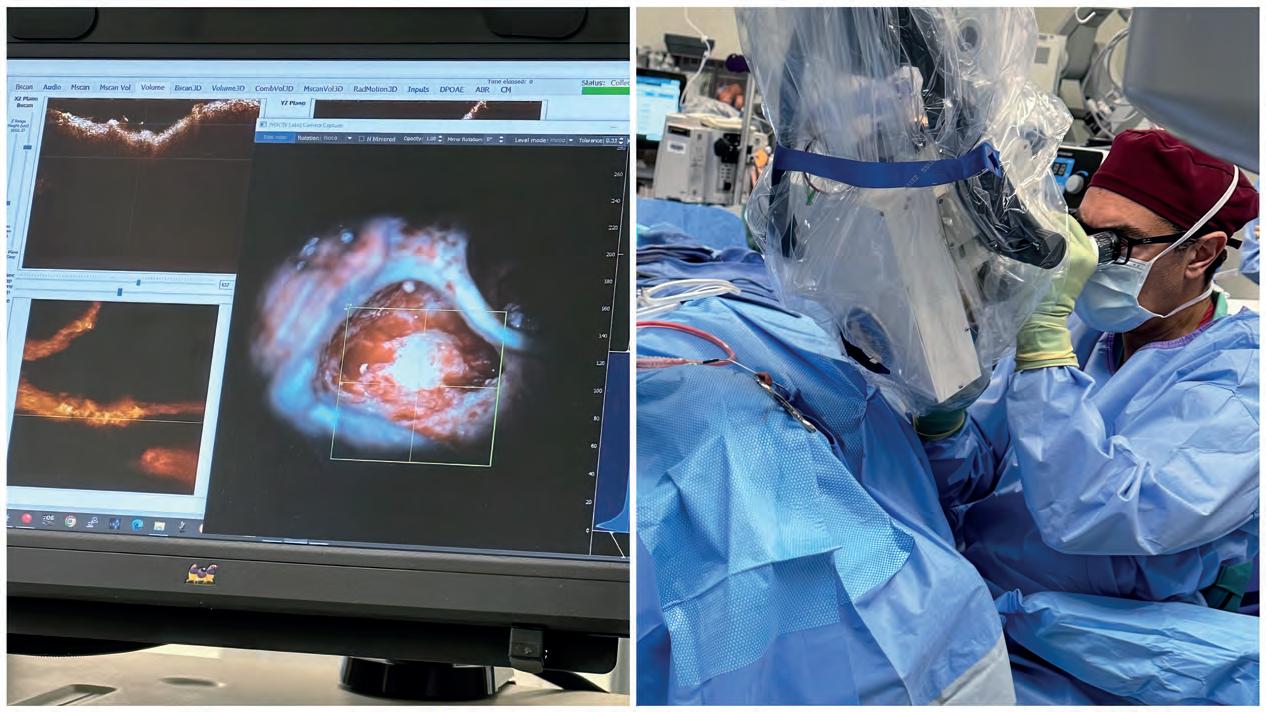
A clearer view
Ear visualisation equipment is a vital tool of the trade for audiologists, ENT surgeons, audiometrists and ear health nurses. HPA delves into advances and trends.
Ear examination and access have come a long way since French physician Dr Guy de Chauliac first described and illustrated an aural speculum in 1363 and English surgeon Dr John Bruton devised the inaugural otoscope in 1862 combining an ear speculum with a perforated mirror and a magnifying glass.
Today’s otoscopes are advanced pieces of equipment which enable precise assessment of the ear's internal structures for inflammation, abnormalities, fluid, wax and other issues.
Likewise, surgical microscopes, endoscopes and exoscopes (robotic microscopes) enable incredible visualisation and access. They include AI-supported systems which feature digital imaging for neurotological interventions such as acoustic neuroma, and advanced visualisation systems for middle ear procedures and cochlear implant surgeries.
University of Melbourne lecturer, audiologist Mr Dominic Power, has taught ear examination skills to audiology students since 2001 and is lead audiologist at its Melbourne Hearing Care Clinic, where audiologists deliver care to patients while training students.
Additionally, he teaches cerumen removal assisted by the VoroTek O Scope, invented in Australia specifically for ENT and audiological work. Power uses it as a teaching and in-practice tool for wax removal and deep canal procedures as it combines LED illumination with a unique optical pathway for looking in ear cavities.
Power says the main change in otoscopes in the past two decades has been LED bulbs which are brighter, drain the battery less and are more reliable. “In the old days audiologists would be mid-way through a session using an otoscope and the bulb would go without warning,” he says. “You’d have to scramble to find a new one.”
LED bulbs don’t colour the ear as much
as incandescent bulbs, he adds. “If you're looking in the ear, you want to make sure wax looks like wax, skin looks like skin, blood looks like blood, and if you’re trying to differentiate one from the other, having a good neutral light source means it doesn't all look white or brown,” Power says.
BENEFITS OF VIDEO OTOSCOPES
Video otoscopes have also changed ear visualisation displaying what’s happening inside the ear on a screen during examination for practitioner and patient to see. Melbourne Hearing Care Clinic has 12 video otoscopes, Power says, adding they’re a worthwhile investment for audiology clinics.
“They’re $3,000 to $4,000 each but we use quality ones which have really good light,” he says. “They're easy to handle, have good attachments that are easily cleanable and are much better compared to video otoscopes released a dozen years ago which were clunkier, needed a separate light source, and were more cumbersome.”
Video otoscopes provide digital images of the patient’s ear which are easily stored in their clinical record for future comparison and consultation with other audiologists or ENT surgeons. “We can email them the
picture and ask for a second opinion which is really helpful,” Power says.
“Patients love to see inside their ear and it’s a great educational tool. If they’re cotton bud users, we can take photos of the damage they’ve done and show them. We can also show them if there’s fluid, or why a bit of wax in the ear is good.”
Another tool, Bebird video otoscopes available on Amazon for about $80, connect to a phone via WiFi and an app. They have a bright light and camera to pop in the ear and are more for consumers than practitioners.
“Our audiologists and students have taken them to Cambodia and Thailand to provide advice on ear conditions in remote areas but they’re also helpful for clients with ear conditions who need ongoing monitoring,” Power says.
“Clients can take pictures at home and send images to their doctor or audiologist
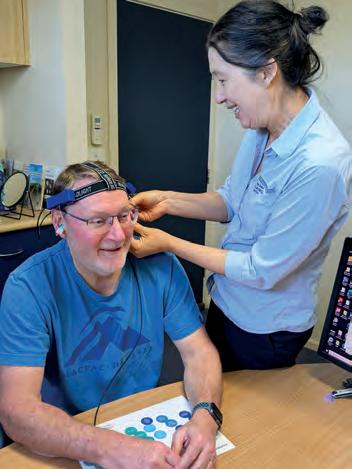
NSW audiologist Alison Chiam using an otoscope.
University of Melbourne audiology lecturer, Dominic Power.
ENT surgeon Prof Payal Mukherjee using a 3D head-mounted exoscope (RoboticScope). Ear visualisation is on the screen.
Image: Alison Chiam.
Image: Dominic Power.
they need to be looking for,” Power says.
Audiologists who fit Lyric invisible hearing aids use an operating microscope to provide clear illumination and visualisation up to the eardrum, providing gold standard visualisation, he adds.
and adult specialist before opening her own practice, Jervis Bay Hearing Centre, NSW, in 2002.
The newest kid on the block in Australia is the WaxScope from the UK which is connected to a phone, and Power believes will complement existing technology. He says the WaxScope has an “additional brilliant light source”, and a nice set of optics to focus at any depth along the ear canal at the swipe of a screen.
FUTURE PREDICTIONS
Brightness is constantly increasing such as fibre optic light sources in Bebirds, the WaxScope, and from LED globes, Power says. He predicts otoscopes will become brighter, smaller and more affordable.
Audiologist of 33 years, Ms Alison Chiam, says “ear visualisation is the foundation of
She says otoscopy and tympanometry remain her foundations. “I have an otoscope that looks the same as when I first started but viewing the ear and eardrum has expanded using existing mediums in a new way; with greater magnification or adding digitalisation including image capture through video onto a screen as a still or moving image, binocular, sound (immittance), pressure, microscopic or electronic detection mediums,” she says.
“Otoscopes are still essentially a light source guided down the ear canal by a funnel shaped tip helping us visualise and examine the condition of the canal and eardrum.
“Audiology clinics have embraced some or all of these technologies and many integrate them with other digital technologies to send, save, record and communicate images.”
DETECTING PATHOLOGY
Projecting something tiny that’s not illuminated onto a screen helps practitioners see markers and points. “You become better at diagnosing pathology, especially pathologies that need to be managed, like cholesteatoma,” Chiam says.
“Video otoscopes are fantastic in powering up our ability to detect pathology early, train colleagues and patients, and bring in expertise and communication”.
Digitalisation means audiologists can share what they see and measure across teams and borders. “I can communicate with my surgeons, share videos and images, ask for advice, and discuss cases with specialist interest groups or a university on the other side of the world and that's huge.
“Conversely, an expert can sit in front of a global audience and show and tell, this is what a cholesteatoma looks like, or what an eardrum looks like when it's oscillating with a tiny tonic tensor tympani or stapedial tendon response.”
“What is most important though is empowerment and education of patients. When a patient sees a giant blob of wax or a hole in the eardrum, they're motivated and understand why we’re sending them for that medical appointment,” she adds.
“The fascination of seeing inside a part of their anatomy they never ordinarily see adds understanding and personalisation to the diagnostic and rehab process.”
Chiam uses different technologies for different purposes. “My VoroTek Voroscope I love for wax removal. The narrow visual axis and binocular view help me move with finesse and accuracy in a small, deep space.
“I also use it in ears where I need that extra bit of clarity and depth to help grasp what’s happening especially when trying to understand audiograms with possible middle ear pathology such as cholesteatoma.
“Additional diagnostic power and confidence in these tricky cases can help early detection and diagnosis.”
Capturing images has expanded into manufacturing through digital scanning. If Chiam does an ear scan using a 3D ear scanner to provide an impression for a hearing aid or custom earplug, it’s emailed to a manufacturer immediately, reducing turnaround. Scans are saved on her database for a quick replacement if a patient loses a device.
Using pressure is another way to visualise movement of the eardrum. Chiam’s liaising with a university professor in France to provide data assisting in standardising and tuning a pressure sensor for objectively measuring movement of middle ear tendons. Adding machine learning to imagery also scales up diagnostic skills through apps that help visualisation. For example, the University of Pittsburgh free iPhone app – Pitt CMU iTM – uses AI to accurately diagnose acute otitis media. It assesses a video of the eardrum captured by connecting an otoscope to a smartphone camera.
Ear Science Institute Australia scientists using a video otoscope and viewing images on the screen.
Alison Chiam standardising and tuning a pressure sensor for objectively measuring movement of middle ear tendons.
Image: Ear Science Institute Australia.
Image: Alison Chiam.
Image: Payal Mukherjee.
use a digital video otoscope to capture images which the app analyses and triages.
DIFFERENCE BETWEEN DEAFNESS AND HEARING
In Chiam’s clinic, recent cases highlight the importance of visualisation technology – and an ability to act on what’s discovered.
She recently saw a patient with profound sudden sensorineural hearing loss. “Six months ago, his GP treated him for otitis media and flu and didn’t organise audiology. It’s possible AI imagery recognition could have helped this GP and with more accurate diagnosis, this patient may have received steroid treatment within the window needed for possible recovery," Chiam says.
“Now it’s total hearing loss and I’m referring him for surgery for a cochlear implant or bone-anchored hearing aid so the difference in outcome is huge.”
She was recently in theatre during a cochlear implant for a patient with total hearing loss and a tumour entwined around the auditory nerve in his better ear. His dead ear was implanted, and an excellent outcome was needed, knowing he would go deaf in the other ear.
“With the Cochlear SmartNav navigation tool we could watch on an iPad screen and guide in real time the implant being slowly inserted so there’s less trauma, and we could see each electrode’s response being activated and tested,” she says.
“I could send myself results for each electrode I measured during surgery, ready for the patient to attend ‘switch on’ in my clinic. He’s performing exceptionally well very early on. For compromised patients, every little bit counts, and this visualisation technology played a role.”
TRENDS IN ENT SURGERY
In ear, nose and throat (ENT) surgery, exoscopes, also called robotic microscopes, are making headway. An exoscope is a
digital, high-definition camera system that provides a high-resolution, magnified view of the surgical field to external monitors, offering an alternative to traditional operating microscopes.
The exoscope's optical scope sits outside the patient's body, not requiring the surgeon to look through eyepieces, allowing for a broader field of view and better ergonomics. This reduces the need for surgeons to maintain uncomfortable positions for extended periods.
The team can see the procedure on large screens as the camera captures the surgical field and transmits images to high-resolution monitors. Many exoscopes offer 3D capabilities, providing a realistic representation of depth and anatomy.
The system is often mounted on a robotic arm and controlled by the surgeon with a foot pedal, offering hands-free navigation. It can also be worn as a VR type headset. Improved visualisation is enabled through a broader and brighter image, allowing surgeons to navigate and see structures around the corner.
Sydney ENT surgeon Professor Payal Mukherjee says it’s an exciting time with changing technology. She’s a big advocate for exoscopes and is pushing for hospitals to fund them due to healthcare workers, particularly surgeons, having the highest rates of work-related musculoskeletal injuries. This is because they look down for extended periods through standard surgical microscopes, causing neck and back strain.
The public health system spends a decade in costs and skills to train a medical graduate to become a surgeon, yet their careers are often cut short due to these injuries, she adds.
“Ear surgeons and other microsurgeons use microscopes for long periods causing injury to their necks and backs as they’re hunched over for hours,” she says. “This impacts patient safety – if a surgeon operating on you
is in pain and distracted, they're not going to be able to do the best surgery.
“Many senior surgeons need back and spine surgery due to operating; hospitals have a duty of care to patients but also to doctors." Prof Mukherjee says to get funding approved for very expensive equipment at hospitals for your specialty is a barrier. “But this activity is limiting the life of the surgical workforce. Funding this equipment is in the best interests of surgeons, hospitals and patients,” she adds.
With colleagues, ENT registrar Dr Ankit Ajmera and physiotherapist-turned-ENT surgeon Associate Professor Raewyn Campbell, Prof Mukherjee performed a study at Sydney Adventist Hospital in 2025.
They compared a new 3D head-mounted exoscope with a standard fixed operating microscope and found the exoscope resulted in less musculoskeletal strain, reducing the risk of musculoskeletal injury from high to moderate.
“Visualisation was equivalent to the operating microscope but immediately, we were sitting neutral, were more comfortable and not in as much pain,” she says. “The VR-type headset meant a lot of eye control with your eyes looking up or down controlling zoom, magnification and focus.”
A lighter headpiece would improve comfort, she adds. Other things that could help include hand rests for surgical chairs to rest elbows and arms on, reducing fingertip tremor, important for operating in the ear’s tiny space.
Prof Mukherjee says surgical equipment was traditionally made for men, but more women are surgeons now who tend to have smaller hands and be shorter. Women’s bodies must fit into men’s surgical equipment which doesn’t consider changes with pregnancy or menopause, she adds.
“Different microscopes have different pluses and minuses and we’re running a workshop in February at Sydney Adventist
Prof Payal Mukherjee is more hunched when using a standard operating microscope (left), increasing risk of muscukoskeletal injury, than an exoscope (right).
Image: Payal Mukherjee.
Adj/Assoc Prof Rob Eikelboom.
Image: Ear Science Institute Australia.
microscopes,” she says.
“There are numerous exoscopic systems. The one we studied was a robotic system but others have lighter goggles which are the same idea and disconnect the head from the visualisation field.
“There's lots happening in this space and even in the past 12 months, we've seen other companies bring out different varieties of the same concept. Device companies that look at visualisation are really exploring this as an unmet need.”
Prof Mukherjee says other systems incorporate augmented reality which overlays 3D anatomy in the visual field so you can see critical structures appearing.
TELEAUDIOLOGY ADVANCES
Telehealth is another advance making inroads into ear visualisation especially in remote areas, says Ear Science Institute Australia research manager, Adjunct Associate Professor Rob Eikelboom. He initially worked at Lions Eye Institute in image processing and analysis of the retina and optic disc via telehealth before moving to Ear Science in 2001.
Most of his work for the past 24 years has been in hearing outreach and epidemiology in East Pilbara, looking at the health of the population, association of hearing loss and tinnitus with other health conditions like mental health, and device use.
Video otoscopes have been useful in remote areas, he says. “Parents, carers, kids and their classmates can see what’s happening inside their ears which is great because it takes away the fear factor,” he says.
“It’s a great educational tool for showing wax or a hole in their eardrum compared with their other healthy ear; here's a sign that you used to have a bad ear infection and it's healed or here’s wax we can't see through, so we need to have it cleaned.”
Images have been shared with nurses and ENT surgeons in Perth and elsewhere to ensure correct diagnosis and treatment.
remotely and sends images to a specialist elsewhere – will grow.
While the technology’s great, it’s the people that make the system work, he says. “I’ve seen equipment sitting in a cupboard because nobody knows what to do so it's all about people's willingness to pick it up and have a go,” he adds.
Ear Science also has a Zeiss operating microscope and a VoroTek O Scope in the Pilbara to boost visualisation especially for wax removal.
Adj/Assoc Prof Eikelboom would love future technology to look through the eardrum and into the middle ear. AI or machine learning to detail what an image is would also be beneficial, he says.
“These
“Computer aided diagnosis of what the picture is showing, answering if there is disease, wax, an eardrum hole and how big it is, or if there’s scarring, could be complemented by what audiologists measure using tympanometry to build a picture of what’s happening,” he says.
Brian Applegate, developed a hand-held portable device integrating high-resolution OCT with a traditional otoscope. This allowed clinicians to view the surface and deeper structures of the tympanic membrane and middle ear.
OCT uses light waves to scan tissue and create 3D images, similar to how ultrasound produces images using sound waves. But it produces higher-resolution images than ultrasound, making it a safe option with no risk to hearing or balance.
The researchers claim it is a significant step forward in imaging technology for ear health and could readily fit into the hearing clinic workflow, providing relevant new information for diagnosing and managing tympanic membrane and middle ear disease. Tests on more than 100 patients in a
findings are exciting as hearing loss can happen suddenly and we often don't know why. OCT offers a way to explore the underlying cause and potentially guide treatment." Professor John Oghalai.
“I think more people should use video otoscopes in clinics because they’re a fantastic teaching tool for patients.”
Adj/Assoc Prof Eikelboom is also an advocate for more GP training in otoscopy especially video otoscopes as they’re user friendly and not “in the patient’s face as much”. “Seeing an image on a screen is a distraction for a wriggling one-year-old,” he adds.
IS OCT THE NEW FRONTIER?
Also on the horizon to improve ear visualisation is OCT (optical coherence tomography), a non-invasive imaging tool used in ophthalmology and optometry to produce 3D images of the back of the eye.
In 2024 University of Southern California
clinical trial demonstrated its ability to reveal pathological features previously invisible using standard otoscopy. Clinical applications included monitoring myringitis, tympanic membrane perforation healing, retraction pockets, and subsurface scarring air pockets.
In 2025 the team fitted an OCT device onto an operating microscope to take images during surgery of tissues and cells in the inner ear through the dense bone that surrounds it. It reliably detected fluid imbalance in the inner ear, correlated with hearing loss severity.
“These findings are exciting because hearing loss can happen suddenly, and we often don’t know why. OCT offers a way to explore the underlying cause and potentially guide treatment,” Prof Oghalai says. He hopes it will lead to better understanding of pathology of Menière’s disease, sudden sensorineural hearing loss, cochlear hydrops, autoimmune inner ear disease, and vestibular schwannoma tumours.
Images: John Oghalai.
A screen displays OCT images (above) taken during surgery by Prof John Oghalai (right).
Word of mouth recommendations from someone you know and trust are usually the most valuable. That was definitely the case for Melbourne ENT surgeon Dr Sherryl Wagstaff, who took a colleague’s advice when it came to arranging an audiometric room for her new clinic.
Dr Wagstaff graduated 25 years ago and despite a long and successful career in otolaryngology, had never arranged installation of an audio room. When she needed one for her new clinic, Adeney Clinic in Kew, she decided to investigate properly.
She researched online, asked an acoustic engineer friend for recommendations and met with people from several companies who came to look at the space.
But it was a recommendation by a colleague from Neurosensory - a specialist hearing aid company - that led her to ADF Industries and its managing director, Mr Jono Davies, who has decades of experience in the audiometric rooms’ field.
“Neurosensory had high-quality booths and a company it used in Queensland suggested I contact ADF,” Dr Wagstaff
recalls. “They recommended Jono to me and from the moment I spoke to him, I knew he was the person for the job.
“He was extremely knowledgeable – has exceptional knowledge of the industry –and was helpful, friendly and competent. I did get quotes from other companies which were in the ballpark of the ADF figure but once I spoke to Jono, there was no other choice.”
WINDOW IN THE ROOM
Dr Wagstaff says she even looked at prefabricated rooms elsewhere and went down every acoustic pathway.
“My situation was a bit unique because my clinic is in an old house and there was a room it had to go in, so the fact ADF custom-made the room made a huge difference,” she adds.
Davies came to see the space and said it wouldn’t be a problem – he even checked the foundations of the old house to make certain the stumps could take the weight.
“He did all the measurements and was efficient, advising what he could do that I wanted,” she says. “I wanted a window in the room because there was already a window there, and I always felt that
audiological rooms were claustrophobic.”
The existing window was double glazed, and Dr Wagstaff needed to ensure the new window didn't compromise sound quality. Davies made a double-glazed window in the room that matched the existing window.
“My audiologists Elizabeth Winton and Natasha Bolch who do the hearing tests love that they have a window in their room,” Dr Wagstaff says, adding that she is also extremely happy with the result.
“Patients, particularly those who've had audiograms elsewhere, have been extremely complimentary about the window because previously they always felt claustrophobic.
“Those who have had them done in shopping centres can't believe how quiet it is in the room. The sound was measured independently to ensure it complied to Australian standards.”
Dr Wagstaff has been in many audiometric booths and rooms over the years.
“There are some good, high-quality rooms but I have been in ones where you can hear cars going by and the audiologist has to compensate for that by deducting a few decibels here and there,” she recalls.
The audiometric room featuring a double-glazed window, LED strip lighting, positive dual compression door seal and a high-performance noise reduction panel system with a hidden air-conditioning system.
Image: ADF Industries.
“With Jono's room and my audiologists, I know the tests I'm getting are exact.”
There was a choice of colours and carpets and, again, Davies’ guidance was spot on, including advising against a bright colour which looked nice on paper, but for a smaller area might be too much for an audiologist to tolerate all day.
“It was hard not to be attracted to the bright colour, but he was good at giving practical advice,” she adds.
Little extras added to the high-end finish, such as strip lighting to provide ambience and a hidden custom air-conditioning system.
MINIMAL INSTALLATION TIME
Skilled ADF staff constructed all of the room off site in the company’s Seaford manufacturing facility, reducing the amount of time needed on site. This enabled them to transport it and install it in just four days, minimising interruptions to patient consultations.
“Jono was extremely accommodating in not wanting to do the build when I had patients,” Dr Wagstaff says. “I cleared my Thursday patient schedule so his staff could work on Thursday, as well as my non-clinical day Friday, and they also worked Saturday and Sunday. I only had to clear a small amount of time from a clinical point of view.”
smoother than I thought it would be,” Dr Wagstaff says.
Davies was happy to work with her electrician instead of providing his. In fact, their relationship continues as the electrician works on home cinemas and heeds Davies’ soundproofing advice.
“Their communication with each other was fantastic,” Dr Wagstaff says.
Her personal assistant said the ADF workers were the most polite and respectful tradesmen she had come across; they even cleaned up and vacuumed. “They didn't leave trip hazards, and it was installed in the time frame that they promised,” Dr Wagstaff adds.
They also knew the equipment audiologists would be using and where power points should be installed, reducing the need for her to make every decision, simply requiring signoff.
TURNKEY PROJECT APPEALED
The process was easy, and the fact it was a turnkey project from start to end was appealing, as was not having multiple groups involved, she adds.
Much of this can be attributed to Davies’ can-do attitude, knowledge and expertise in the industry, which stem from the legacy of his family-owned business. He proudly relayed the story to Dr Wagstaff of how his father Mr John Davies founded the business more than 40 years ago and installed his first audiometric room 30 years ago.
Since then, ADF Industries (All Duct Fabrications) has grown to design, manufacture and install hundreds of custom-made audiometric rooms, micro and modular booths and test laboratories across Australia and the world. Its quality products feature in audiology and ENT clinics, hospitals, at mining sites and in mobile hearing testing vehicles worldwide.
All are engineered and built to Australian or international standards as required to provide an optimal level of ambient sound, producing lab-type conditions to perform hearing tests.
Dr Wagstaff is originally from country Victoria and attended Maryborough High School before graduating in medicine from Monash University and doing surgical training at The Alfred Hospital.
“Jono has exceptional knowledge of the industry and was helpful, friendly and competent. Quotes
from other companies were in the ballpark but once I spoke to
Jono,
there was no other choice.”
Dr Sherryl Wagstaff Adeney Private Hospital
go wherever they send you and after I finished, I did a separate fellowship at The Royal Victorian Eye and Ear Hospital and the Royal Melbourne Hospital in cochlear implants and acoustic neuromas,” she says.
She then did a 12-month stint in the UK on acoustic and skull base surgery at Addenbrookes Hospital, Cambridge.
Back in Australia, Dr Wagstaff worked at several hospitals as a visiting medical officer before becoming head of the ENT unit at Eastern Health in Box Hill and then medical director at Epworth Eastern Private Hospital.
NO GAP HOSPITAL
She is now medical director at Adeney Private Hospital in Kew, Australia’s first private hospital to provide zero out-of-pocket costs across its full suite of hospital services for people with Medibank or Bupa health insurance. Her subspeciality interest is otology.
The hospital operating entity, which is 51% owned by more than 40 doctors including Dr Wagstaff and 49% owned by Medibank, opened in March 2025. Her private practice where the audio room was installed, Adeney Clinic, is associated with the hospital.
In 2024 when the room was installed, she was organising a charity ball for the hospital. “Jono was interested in that and even came along,” she says. “He really is a beautiful person.
“I would have no hesitation in recommending him and ADF to any audiologists, ENTs or anyone else who's putting in an audiometric room or booth.”
*For more information see adfindustries.com.au/
Audiologist Liz Winton performing hearing testing in the audiometric room.
Image: Adeney Private Hospital.
Image: Sherryl Wagstaff.
Specsavers says it has revolutionised screening with its free 15-minute checks.
A successful model
In the eight years that Specsavers Audiology has been in Australia, its staff have conducted 4.63 million hearing screenings, changing the landscape of how people access hearing checks and treatment.
Mr Tom Craw, managing director – audiology at Specsavers ANZ, remembers hearing about the “unattainable triangle” during a marketing class at university. Price, quality and service sat in different corners.
“The lecturer said you could only ever achieve two,” he says. “But that unattainable triangle is attainable for Specsavers –we've got great quality, great prices and great service.”
Sometimes he thinks he would love to go back and show that lecturer how Specsavers achieves all three through its innovative model of joint venture partnerships.
Craw has been with the organisation for 18 years – the entirety of its journey in Australia – having started in 2007 before the first optics store opened in 2008. An accountant, he is now executive director and managing director of audiology for Specsavers Australia and New Zealand.
He’s proud of many things that Specsavers Audiology has achieved in both countries but one that stands out is the way it has transformed hearing aid accessibility and affordability.
“Many Australians and New Zealanders previously thought hearing aids were out of reach but we’ve changed that,” Craw says. “Removing those barriers for customers to provide accessible value, care and great clinical expertise to all, it's our model.
“I’ve seen this vision come to life firsthand over the optics journey and continue to see it in audiology.
“Specsavers aims to expand audiology services to all 395 Australian optic stores – we’re in 82% but over time, we'd love to be in 100%. That’s the goal, along with not having a Specsavers optometry or audiology customer, but a Specsavers customer.”
Craw stresses: “While 4.63 million screens are amazing, it's not just a great number; it's the amount of lives changed off the back of that which is the more incredible aspect.
“A significant number go on to a full assessment and are fitted with hearing aids.
“Many probably never considered a hearing check or doing something about their hearing loss so the convenience of having a test while there for an eye check is a huge step.
“We're also seeing more awareness of earlier intervention and better outcomes." Through screening and earlier intervention, he says Specsavers gets a chance to dramatically reduce the seven-to-10-year lag between someone recognising they have hearing loss and doing something about it.
“We plant the seed so even if they’re not ready to contemplate anything immediately or if they don’t have hearing loss, as they return for eye checks, they repeat the test and conversations about hearing loss
Specsavers Australia is a pioneer of hearing
“We don’t even offer screening elsewhere; our UK audiology business is 21 years old, and it doesn’t operate like we do," he says. "We’ve embedded it from the start in Australia and New Zealand as a key plank of
Offering screening is also a drawcard for this increasingly health-conscious
“We’ve revolutionised screening in this industry with our free 15-minute hearing checks which a lot of the wider industry now
He says research suggests longer term impacts of not acting on hearing loss include social isolation, depression and loneliness.
“The scientific data is quite significant so we can make a difference by getting people onto an earlier journey,” he says.
Specsavers has been good for Australians, normalising hearing checks, which is good for the industry, he adds. And Specsavers also offers transparency in pricing with all prices on its website which reveal its competitive advantage.
“We offer the same leading hearing aid technology but commercial benefits of not paying standalone rents, leveraging optometry stores, sharing resources such as reception staff, and global buying power, allow us to provide the incredible prices that we do,” Craw says.
FILLING THE GAP
When pondering the phenomenal growth of Specsavers Audiology in ANZ, Craw attributes the success to the joint venture model where local audiologists, optometrists and retail Partners own and operate their businesses backed by vital support from Specsavers in marketing, payroll, financials and business management.
“The joint venture model is the not-so-secret secret of our success,” Craw says. “It’s about empowering audiology professionals to own and operate their own business with the full support of Specsavers behind them and embedding
“While 4.63 million screens are amazing, it's not just a great number; it's the amount of lives changed off the back of that which is the more incredible aspect.”
Tom Craw Specsavers
an audiology and optometry environment that creates a multi category experience for our customers.”
Craw says leveraging off a recognised optics customer base and following a model that’s been well tested in optometry for 40 years, allows Partners to focus on providing great clinical care and customer service, while Specsavers helps with other areas.
“There was a gap in the market which we filled in terms of providing accessible value backed by great quality products and services,” he adds.
Craw says the industry had been perceived as selling hearing aids to pensioners with a Hearing Services Program voucher at one end, and top of the range devices at the other end.
“It never felt right to me, and I think we've got a great solution for anyone's goals or budget.
We can provide great outcomes for people, and our Partners are conscious of providing the right product for our customers, not just selling top end technology,” he adds.
Specsavers Audiology
has achieved since launching in 2017:
• 4.63 million hearing screenings and 616,655 hearing checks
With net promoter scores (NPS) like Specsavers’ in the high 80s being extremely rare, Specsavers’ dedication to excellent customer service and clinical care is apparent to its customers, he says.
“It's a great reflection of the care and service our staff are providing and satisfaction in terms of price,” Craw says.
“It’s also a reflection of the life-changing value the product can provide because they rate satisfaction with the product –and you don't get an NPS of 88 unless the hearing aids make a significant difference in someone's life.”
It is a business with great purpose, Craw adds. “Some of the stories we hear and the letters of gratitude we receive – people saying it’s saved their marriage or being grateful for being able to hear around the Christmas table – it's incredible when you get that feedback. It gives you great satisfaction when you work for a business with purpose like that.”
CULTURE, PURPOSE AND VISION
While 18 years is unusual in corporate life, it’s the norm in Specsavers, he says, adding that he was drawn to the organisation because of its clear purpose.
“I was one of the first Australians on board – there were 12 of us before we opened the first optics store,” he says.
“I was lucky enough to work with Doug Perkins, one of our founders, for the first three years. I got to understand Specsavers’ incredible culture, purpose and vision.”
The family values of Doug and wife Dame Mary Perkins permeate the organisation. “That culture of treating people as you'd like to be treated, the culture of support, development and inclusion drives our performance and retention of great team members,” Craw says.
Specsavers’ key supply partners invest
• 458,187 hearing aids prescribed
• 192 ,748 audiology customers
• expanding to 324 Specsavers stores
• 188 audiology Partners and 102 clinicians employed
• 70% -77% of staff who voted anonymously in the 2024 Great Place to Work Australia award said it was exactly that; and it was voted a great place to work six years in a row
• A net promoter score (NPS) metric to gauge customer loyalty and satisfaction of 88% in Australia
heavily in research and development.
“We've seen those benefits over eight years, whether enhancing sound quality, connectivity, reducing battery use or, in the past 12 months, a step change in technology with artificial intelligence-trained technology.
“Deep neural network chips in hearing aids with AI have enhanced the ability to separate speech from noise, creating a better user experience," he says.
“It’s something our clinicians and the public are incredibly excited about.
“We’re offering the latest Resound AI hearing aids at incredible prices that everyone can afford which is something we’re very proud of.”
BUSINESS OWNERSHIP
While business ownership isn’t easy, he believes Specsavers lightens the load for its Partners, offering a chance to make that big step with the support of a trusted brand behind them.
“They can develop as clinicians and business owners and get the stimulation and rewards that come with business ownership. They create an asset they can sell in future,” he says.
“It’s a compelling offer in terms of value, care and product quality.
“Our Partners are incredibly well supported as that leap of faith, going into an independent world if you’re a clinician is quite daunting, whether sourcing your own product, doing your own marketing, or bits and pieces that keep you up at night.
“We do that on behalf of our Partners; we find a great product at a great price; do the marketing, supply chain, payroll, financials, HR, legal, all the things that make business ownership hard, so our Partners can concentrate on the clinical side.”
The organisation invests heavily in Partner and team member training.
Audiology relationship managers help Partners with business skills, focusing on commercial acumen, while clinical field teams assist with clinical expertise.
One Audiology Partner is often placed across two stores until demand grows.
“We’re finding that no matter where we go, the success seems to follow," Craw says.
"Australians are loving us being there to assist them with their hearing, and in doing so we’re changing lives through better hearing.”
Deep neural network chips in hearing aids with AI have enhanced the ability to separate speech from noise, creating a better user experience.
Images: Specsavers.
Audiology is now in 324 of Australia’s 395 Specsavers stores.
The allure of better hearing
Widex has launched its new W1 chip in Australia, debuting in innovative Allure hearing aids. The company says Allure processes sound up to 16 times faster than competitors, delivering more precise hearing.
Precision is the theme of the new Widex Allure hearing aid launched at roadshows around Australia in September 2025. Its featured Precision Hearing Technology suite boasts precise sound processing, noise management and adaption.
This delivers natural, pure sound, which focuses on clarity, says audiologist Mr Peter Mckinnon, head of commercial acceleration for WS Audiology. Combined with new world-first cloud-based fitting software, it provides natural sound that sounds great in every situation for people with hearing loss, he adds.
Widex is a premium Danish brand that has existed for more than 65 years. Its vision focuses on sound quality, with the goal being hearing aids that sound so natural that people forget they’re wearing them.
“Widex has a unique way of processing sound,” Mckinnon says. “We want sound to be pure, accurate and complete with a focus on precision sound processing. Part of this is the speed of processing.
“Allure hearing aids process sound 16 times faster than our competitors which is important, particularly for people with mild
LOWEST RETURN RATE
This focus on sound quality delivers many benefits, Mckinnon says, as exemplified in a recent survey of 246 hearing care professionals who compared their experience with six brands.
“Widex had the lowest rejection rate for first time wearers which is important as you only get one chance to make a first impression,” he says. “People don't want hearing aids and generally wait seven to eight years before getting them. They’re a reluctant purchase so you want to make the experience as positive as possible.”
Wearers of Widex devices also had the least follow-up visits and there was less fine tuning required, the survey found.
Mckinnon explains digital processing of hearing aids can be done in the time domain or the frequency domain, but Widex is the only brand that processes in the time domain: this is said to deliver faster and better sound quality.
Despite being a challenge, the company chose to do it this way because it is Widex's vision. “We don't want to compromise on natural, sound quality,” he adds.
The W1 chip is four times faster than
The marketing campaign tagline – ‘the difference is clear’ – plays to the fact that the device focuses on clarity, and this is its point-of-difference.
“Underlying our Precision Hearing Technology are precise sound processing, precise noise management, and precise adaption,” Mckinnon says.
PRECISE SOUND PROCESSING
Precise sound processing, the flagship feature, is about the speed of processing. It features technology called Zero Delay Processing.
“When the sound is picked up by the microphone on a standard hearing aid, it takes a bit of time to process before it comes out of the speaker into the ear,” Mckinnon says.
“The greater the delay, the more distortion you'll get particularly with open fittings. This is because the sound going through the hearing aid combines with the sound coming through the vent. When these two paths meet, if they are not in sync, it causes distortion.”
This is why faster processing is critical when it comes to sound quality, he adds.
“Normally, our competitors’ standard hearing aids have a delay of about eight milliseconds, which is not long, but it does create some distortion, while our pure sound and Zero Delay technology have a delay of half a millisecond,” he says.
Widex had a version of this technology in its previous platform, Moment, but it was only suitable for mild hearing loss and in quiet, less complex environments. Allure, however, is fully adaptive so can be used in any situation, including challenging noisy environments, he adds.
Advanced features including noise reduction and directional microphone technology are designed to work in every environment. “The key message is people benefit from this natural sound, and it sounds great in every situation,” Mckinnon says.
Above: Widex Allure receiver-in-canal (RIC) R D hearing aids in autumn beige.
VIPs and Widex staff attending a Widex Allure pre-launch event.
“It can be used for a greater range of people, up to those with moderate hearing loss. When there’s more severe hearing loss which generally doesn’t utilise open fittings, the level of distortion becomes less important because the cochlea is quite damaged so improvements in sound quality aren’t as noticeable.”
PRECISE NOISE MANAGEMENT
Hearing aids must understand the environment to determine how to optimally emphasise speech and manage noise in a natural way.
“As we go about our day, the acoustic environment changes constantly, it's dynamic. We need to precisely understand that so we get the balance right between speech enhancement, but also manage noise so we can hear it and it's not uncomfortable and doesn’t affect speech understanding or drown things out,” Mckinnon explains.
A new feature, Speech Enhancer Pro, provides this precise understanding of noise in the environment using 52 band input noise analysis.
“Measuring the noise so precisely in 52 discrete bands means we have better understanding of noise in the environment so we can adapt better because it's all about optimising balance between speech and noise,” Mckinnon says.
“Some systems can be too aggressive, and noise is reduced too much so it sounds like you're inside a barrel, it's artificial, but if you don't reduce noise enough, it compromises speech.”
IMPROVEMENTS IN MUSIC CLASSIFICATION
Precise adaption is the next feature. Allure’s sound class technology fully adapts to the always changing environment, or soundscape, in a natural way, constantly classifying the environment so it can adapt device settings.
“One area that has really improved with Allure is music classification. This can be challenging because many hearing aids assume music is noise and suppress it,” he says. “A new beat detector sensor more accurately detects music and it’s also more natural and people hear what they want to hear.”
Allure’s higher end devices can even distinguish different types of music –classical versus pop – while the lower end can detect that it’s music.
The Allure RIC RD is a lithium-ion rechargeable device at four performance levels – premium, high end, mid-range and entry level. “It’s a nice-looking device, elegant, typical Danish design,” Mckinnon adds.
Plus, there are three chargers – Standard, Charge and Clean, and Portable.
“Charge and Clean cleans and dries the device as it’s charging, adding value by improving longevity and dehumidifying,” Mckinnon says. “The dry and clean chargers
are fantastic in dehumidifying hearing aids and reducing the risk of corrosion especially in humid North Queensland.”
The portable charger, within a hearing aid case, has an internal battery that provides a full week’s charge without having to connect to mains power.
The new Allure hearing aids are supported by an upgraded smartphone app. The Allure App allows wearers to remotely adjust features in their Allure hearing aids including volume, programs and frequency response. “The app focuses on helping wearers get the most out of their hearing aids, particularly first-time wearers, and is designed with accessibility in mind including contrast adjustments to see controls better,” Mckinnon says.
The Allure App also features upgraded AI support. In environments where the wearer would like to personalise the sound, AI in the app optimises sound quality by communicating with the cloud.
Based on the experiences of hundreds of thousands of wearers worldwide in similar environments, it recommends settings which have been proven to improve wearer satisfaction. Several options are AI-generated, with the opportunity for the wearer to choose the best one.
“Hearing aids are often first fitted in a relatively quiet clinic,” McKinnon says. “We all know that what sounds good in quiet, may not sound ideal in other situations including noise. Instead of returning to the clinic for fine-tuning, wearers can utilise the power of AI in the Allure App to make real-time, real-world adjustments to the hearing aids themselves”.
The app supports Bluetooth connectivity and has a dedicated streaming compressor that processes sound from music differently than speech, again providing better sound quality for streaming. Battery life of 26 hours includes five hours’ streaming.
CLOUD-BASED FITTING SOFTWARE
Hearing care professionals usually fit hearing aids using software on a PC to program clients' devices
“With Allure, we’ve introduced the world's first cloud-based hearing aid fitting system, Widex Compass Cloud,” Mckinnon says. “This has many advantages.
“Normally when we add features, we send out new software and have to ensure the clinician installs it, but we’re constantly adding features and functionality, so being in the cloud means it is always up to date.”
Because it’s a new technology and platform, Widex went back to the fundamentals of understanding the workflow, focusing on simplicity and streamlining to make it easier to fit, and to achieve a great and precise first fit.
“We worked in collaboration with a lot of hearing care professionals in developing this workflow over many years,” Mckinnon says. “We’ve noticed since launching in the US and some European countries in July 2025, that Allure’s focus on sound quality and the cloud software mean people are needing less fine tuning.
“In the longer term, we're trying to build a digital ecosystem called All in One Audiology, like a portal that supports fitting and ordering support, all in an online platform. We've started with fitting, because that's core, but over time, there'll be additional services and support so we're truly future ready with Widex Compass Cloud.”
*For information, see widex.com.
Internal connections in the WI chip.
Images: Widex.
The WI chip inside Widex Allure hearing aids (left). And the Widex Allure RIC R D hearing aid in tech black.
Helping hands for ears
A volunteer trip by Australian audiologist mates SANDRA LEE and SACHINTHYA DONA has had a big impact on hearing services in Fiji including upskilling staff, supporting a hospital ear health department launch and adapting the Kendall Toy Test to a local language.
When the “father of special education in Fiji”, teacher Mr Frank Hilton noticed students dropping out of school because of hearing and vision problems, he decided to do something about it.
Hilton founded Project HEAVEN (Hearing and Vision Enhancement) in 1997 to provide early diagnosis of ear and eye impairment in school aged children across Fiji by providing on site screening services.
In the past 30 years, the project has screened more than 200,000 school children. This dedicated work leads to detection and referral of over 1,400 cases of eye and ear conditions each year including hearing aid fittings and provision.
Hilton, an English teacher who migrated to Australia in 1958, was head teacher at Nepean School for Crippled Children in Sydney before moving to Fiji with his wife Nora in 1967 to become head teacher at Suva Crippled Children’s School. The Hiltons have since dedicated their lives to setting up services and helping local disabled children.
Assisting Project HEAVEN’s work is EARS Inc, an Australian Christian not-for-profit association of audiologists, audiometrists, allied health care professionals and others dedicated to training and equipping health workers in developing countries.
For 27 years, EARS Inc has assisted hearing impaired people to receive help and rehabilitation. These people would otherwise not have the capacity or opportunity to overcome their disability.
“We provide ongoing training and support to local workers at health clinics, hospitals, deaf schools and mission groups in developing countries,” a spokesperson said. “Through this training, our volunteers are equipping local workers with the necessary skills and resources to provide a sustainable local service to rehabilitate people with hearing loss and help them become self-sufficient and independent.”
EARS Inc came about after Mr David Pither, a Melbourne audiometrist, established an earmold laboratory in Vanuatu. He later went on to establish 40 more in low- and middle-income countries over the next 20 years, along with training local teachers and health workers to make earmolds, test hearing and manage hearing aids.
Mr Peter Barlett, a Ballarat audiologist, joined Pither on a trip to the Philippines and they founded Ears Inc in 1998. Despite few volunteers and limited financial resources, thousands of people’s lives have been changed by EARS Inc, most of whom would not otherwise have had access to audiology and hearing aid services.
In 2025, Ears Inc put out a call for audiologists to help with the hearing program in Fiji.
SCREENING, STAFF TRAINING AND A WORLD FIRST
Melbourne audiologist Ms Sandra Lee from Victorian Hearing, and Gold Coast audiologist Ms Sachinthya (Sacha) Dona responded. The pair worked together at Attune Mornington 10 years ago and kept in touch. They aspired to deliver better healthcare in regions of the world that had less and this seemed the perfect opportunity.
They planned the trip for June 2025 through Ears Inc’s audiologist member Dr Donna Carkeet, who has dedicated many years with Ears Inc and is the regular audiologist in contact with Fiji.
In Fiji, Lee and Dona contributed to screening programs and staff training, focusing on empowering local healthcare workers to build long-term capacity. They also brought a refurbished donated tympanometer and trained staff in
tympanometry, air and bone masking and air conduction school screenings.
Lee says Project HEAVEN projects rely on funding and grants and when there’s none, workers must stop work until the next round of funding.
“With the help of Project HEAVEN and our local Fijian workmates, we achieved a world-first culturally appropriate adaptation of the Kendall Toy Test (KTT) into the local iTaukei language, one of the most spoken languages in Fiji,” Lee says.
“This milestone will help bridge gaps in paediatric hearing assessments, ensuring more children receive the care they deserve in a culturally meaningful way. This was an exciting achievement.”
The KTT is a speech discrimination test
Hearing screener Luisa Natadra has visited schools in Fiji for 20 years testing children’s hearing.
Project HEAVEN staff, Nilesh, (from left) and Alanieta, with (right) Viniana, and Savu. Sandra Lee and Sachinthya Dona are in the middle.
used in paediatric audiology to assess a child's ability to identify spoken words by pointing to or handing them familiar toys. Performed with visual cues removed, the child is asked to "show me the [toy's name]" as the words are spoken at varying, quiet sound levels to determine their hearing threshold.
“Local nurse Akanisi travelled 1.5 hours to spend two days with us to learn the basics of ear anatomy, middle ear pathology and hearing tests, so she could start an audiology department in Tailevu Sub Divisional Hospital,” Lee says.
“She was in the process of setting it up and we were proud to assist her with the launch of this ear health department.”
The Australians also worked with the Frank Hilton Organization which offers critical services for children with disabilities in Fiji, including early intervention, audiology, speech pathology and physiotherapy.
Working out of the Frank Hilton Organization office, they supported the paediatric audiology program at Fiji’s main public hospital, Suva’s Colonial War Memorial Hospital. They upskilled and trained audiometrist Ms Shabina Dean and hearing aid technician Mr Desmond Tabu.
“They’d started an audiology department and ear mold lab themselves from scratch and to see them make in-house ear molds for children with hearing loss needs was eye opening and resourceful,” Lee says.
“It’s one of only two centres in Fiji that offers hearing aids to the public. The other is an independent audiometrist called Tukana. And there are only two audiometrists in Fiji!”
BOOTH
BUILT FROM SCRATCH
Lee says Dean was a strong advocate for hearing health and rigorous training. Together with her CEO Sureni’s forward-thinking vision, they built Fiji's first comprehensive hearing booth with diagnostic equipment such as TE/DP, OAEs and ABR. They established processes with Dr Carkeet from Ears Inc coaching and guiding her.
“Shabina’s inspirational; her daughter was the first Fijian to receive a donated BAHA surgery via Cochlear,” Lee adds.
The Australians provided hands on and one-to-one training on air and bone conduction masking, troubleshooting and hearing aid training, mainly with behind-the-ear-devices but also ADHEAR non-surgical devices that use bone conduction to help users hear.
Additionally, they assisted with newborn infant screenings at the CWM Hospital and created otoacoustic emissions (OAE) protocols. Dona says they were grateful for the opportunity to contribute to the impactful initiatives taking place in Fiji.
DONATED HEARING AIDS
She says Dr Carkeet dedicated many years to supporting local staff.
“I believe the diverse skills Sandra and
foundation Dr Carkeet established,” Dona says.
“We assisted in refining and streamlining existing processes such as record keeping and patient follow-up.
“One particularly meaningful aspect was being able to put donated hearing aids from our own clients to good use.
"Knowing that these devices could directly improve lives overseas gave our clients the chance to be part of something bigger and it’s a powerful reminder we can share with them about just how valuable access to hearing aids truly is.”
Dona found the experience eye-opening and says it broadened her perspective on what’s possible in audiology.
“I'm excited about continuing to support the dedicated staff we trained, whose eagerness to learn was inspiring and encouraging,” she adds.
Lee says she's incredibly grateful that her employer, Victorian Hearing, believes in accessible hearing heath care beyond its clinic walls and that its clients were so generous with their hearing aid donations.
“It wouldn’t have been possible without them, and the assistance of Ears Inc to connect us to Project HEAVEN and the Frank Hilton Organization,” she says.
“We were told Frank noticed students dropping out of school because of hearing
the years it expanded to school screenings and device fittings.
“To give the gift of hearing and bring over donated medical equipment is remarkable.”
The Australians were also impressed with local hearing screener Ms Luisa Natadra who has visited schools in Fiji for 20 years.
“She recalled stories of the early days when they travelled hours on foot with an audiometer and a generator on horseback to reach remote communities,” Lee says.
“They would push the school tables together, pull a blanket over the top, and rest there for the night before starting a second day of screening.
“To reach some schools even today takes six hours by boat one way. It’s inspiring the work they do.”
OUTREACH GROUNDS YOU
The need is great and it’s sad to hear that when funding runs out, some parts of organisations have to lay off staff until more funding comes through, Lee says.
“They’re always keen to have audiologists visit and teach them so they maintain their clinical skills,” she adds.
“I would recommend outreach to remote communities for any audiologist to be grounded in why it is we do what we do; to help people hear and live connected lives with their community.”
Frank Hilton Organization staff Desmond (left) and Shabina (third from left) with Sachinthya Dona (second from left) and Sandra Lee (right).
Images: Sandra Lee.
Sandra Lee (centre) with Akanisi (left) and Violet (right).
Assisting and enhancing hearing
Hearables and assistive listening devices have exploded onto the market in recent years. Some audiology clinics in Australia are making the most of their popularity, providing another option for clients.
Devices to improve hearing are no longer constrained to the hearing aid category. The rapid rise of hearables and assistive listening devices – or ALDs –is transforming everyday listening. People with no hearing impairment also want an improved listening experience, better communication and the ability to tune in and focus on conversations or tune out of background noise.
Hearables are devices that combine some functions of a hearing aid in a consumer wearable. They are over-the-counter devices not regulated as medical devices. Even so, they’re providing new opportunities for audiologists to differentiate and elevate their service.
One expert, Dr David Sly from Ear Science Institute Australia, believes hearables may comprise about 15% of the Australian hearing aid market. And a recent report predicts sales will reach nearly $2.5 billion in Australia in the next 10 years.
Expert Market Research’s Australia Hearables Market Size, Share Analysis and Forecast Report (2025-2034) estimates the Australian hearables market was valued at $942 million in 2024. It predicts the market will grow at a compound annual growth rate of 10.4% between 2025 and 2034 extending to almost $2.5 billion.
“The hearables market is growing with an increase in the development of wireless connectivity technologies, health tracking systems incorporation, sustainable hearables, and active noise cancellation technology,” the report says.
Earbuds with built-in hearing enhancement that don’t only stream music or calls – but also improve communication, focus, and inclusion – are examples of hearables.
Apple’s AirPods Pro 2, launched worldwide in 2024 and in Australia in 2025, have especially taken the hearables market by storm. They have an in-built Hearing Aid Feature, hearing test and connect to Bluetooth. The Pro 3 version with a longer lasting battery launched in Australia in September 2025.
Many audiologists initially had reservations about the AirPods being marketed as a clinical grade hearing aid for adults with mild to moderate hearing loss as they feared they may lose clients. But some practitioners now realise the devices are creating more awareness
about hearing health amongst the public and act as a gateway to superior hearing aids down the track when people’s hearing loss progresses because they realise the benefits of improved hearing.
This is exactly what preliminary results from a small world first trial of hearables in Australia are showing. Most participants who tried hearables later turned to audiologists for hearing aids.
ALDS AID SAFETY
Hearables are the latest addition to the ALD space, says Hearing Australia’s principal audiologist, Ms Karen Hirschausen.
In her words: “Hearables are earbuds that offer hearing aid-like functionality, helping people hear better in everyday situations. They’re a fantastic option for those who aren’t quite ready to commit to traditional hearing aids.
“Since earbud use is already so common, hearables offer a familiar and stylish way to take that first step toward better hearing without the stigma or formality of medical devices.”
Other examples include homegrown Audeara Buds, marketed as “a listening aid with sound personalised to clients’ hearing profiles”, Bluetooth and Auracast connectivity and a hearing check using the Audeara Tune app.
ALDs are designed to enhance hearing and environmental awareness and can be used with or without hearing aids, Hirschausen says.
A Hearing Australia audiologist fitting headphones.
Earbuds with built-in hearing enhancement that improve communication, focus, and inclusion are examples of hearables.
There are two main types of ALD needs:
• Auditory support: Helping people hear better – whether it’s a conversation, the TV, or a phone call.
• Safety and awareness: Alerting people to important sounds in their environment, like a doorbell, smoke alarm, or someone calling out.
“ALDs achieve this by amplifying sound, or using vibration, light, or notifications to make sure the person is aware of what’s happening around them,” she adds.
“They’re especially helpful in situations where hearing aids alone might not be enough.”
ALD UPTAKE DOUBLES
Hearing Australia offers many ALDs and says they are increasing in popularity.
“TV assistive listening devices are hands-down the most popular,” Hirschausen says. “Why? Because the television remains a central part of home life – and often a battleground for volume control.
“When one person needs the volume cranked up and the other finds it too loud, ALDs offer a peaceful solution.”
Also, as televisions get bigger, people tend to sit further away, which can reduce
sound clarity especially beyond 1.5 metres, she adds. “TV ALDs help bridge that gap, delivering clearer sound directly to the listener without disturbing others,” she says.
“At Hearing Australia, ALD uptake has nearly doubled in the past five years. But it’s not just about more people using them – it’s also about how they’re using them.”
Clients with hearing aids are increasingly choosing devices that stream TV audio directly to their hearing aids, eliminating the need for bulky headphones. This allows them to enjoy their preferred volume without compromising comfort or style, she says.
“We’re also seeing a rise in smart alert systems that send notifications to phones or smartwatches when someone’s at the door or if a smoke alarm goes off – making safety more accessible and modern,” she adds.
WIRELESS STREAMER TREND
Trends include wireless streamers becoming the go-to choice. “They offer seamless connectivity with hearing aids, TVs, and other devices, making the experience smoother and more integrated,” Hirschausen says.
“This trend ties in with the shift toward discreet, user-friendly tech that fits into everyday life without drawing attention or requiring extra gear.”
ALDs sold by Hearing Australia range from headphones that use a health-check algorithm to tailor sound to each person’s unique hearing profile and feature noise cancelling and in-built microphones; to wireless headphones with speech mode that reduces background noise and enhances speech; and kids headphones and in-ear headphones that protect young ears and help curb noise-induced hearing loss with features including a volume restrictor.
Alerting devices include telephone alerting systems, vibrating alarm clocks, doorbells and smoke alarms.
Cordless phones feature easy-to-read displays, emergency call functions and large buttons for easy dialling. Personal amplifiers, pitched as devices for when people’s hearing needs a boost but conventional hearing aids may not be the best option, can be used with headphones or earbuds. They include Roger Select microphones to boost hearing performance.
There are also customisable hand-held or body-worn personal listening amplifiers with Bluetooth connectivity.
HEARABLES STUDY ON MENTAL AND PSYCHOSOCIAL WELLBEING
Hearables may also offer other benefits apart from enhancing hearing.
In Western Australia, audiologist Dr Dona Jayakody and psychiatrist Dr Andrew Ford are conducting a clinical trial investigating whether hearing amplification via hearables, combined with a behaviour activation program, can improve mood and social participation.
nearly doubled in the past five years. It’s not just about more people using them; it’s also about how they’re using them.”
Dr Jayakody began the research while at Ear Science Institute Australia in Perth and is continuing it at the WA Centre for Health and Ageing at the University of Western Australia (UWA).
“We decided to do this trial because our previous work saw an association between untreated hearing loss and depression, anxiety and stress,” Dr Jayakody says.
“We also saw increased levels of social isolation and loneliness in people who have hearing problems. Many patients were telling us they wanted to take their hearing health matters into their own hands and wanted something they could manage.”
Others were concerned about the cost of hearing aids, she adds. “Everyone was talking about hearables, they were coming onto the market and the device we used in the trial was listed on the Hearing Services Program’s device schedule,” she says.
and mental distress that is commonly associated with hearing loss.”
The buds had an amplification function and could be adjusted via smartphone.
Dr Ford is an Adjunct Associate Professor in the UWA Medical School and consultant older adult psychiatrist with North Metropolitan Health Service. With colleagues he has previously investigated the role of behavioural activation in improving mental health outcomes in nursing homes and he uses this therapy in his day-to-day clinical practice.
Dr Ford adds: “Hearing loss can adversely affect someone’s quality of life and contribute to feelings of loneliness, social isolation and even depression.
“Our behavioural activation program focuses on reducing the social isolation
The hearables trial has four groups: one does the behaviour activation program, another receives hearables, a third group has both, and a fourth is the control group.
Assessments were done before the study started and three months after it began.
Participants also had the choice to swap to trialling hearables or behaviour activation if they wanted after completing the first three months in a different group.
The study, funded by the National Health and Medical Research Council, aims to recruit 200 older adults with mild to less than moderate hearing loss who have not used hearing aids or hearables.
Preliminary results are in on the first 50 participants who have completed the program.
“The feedback we've got from people using the hearables is that doing this
Karen Hirschausen Hearing Australia
Image: Hearing Australia.
Image: Ear Science Institute Australia.
Audiologist Dr Dona Jayakody with hearables trial participant Michèle Drouart (right) who said the trial had positively impacted her.
Hearables trial co-ordinators, Dr Dona Jayakody and Dr Andrew Ford. Image: Ear Science Institute
see a health professional such as an audiologist or doctor, with users adjusting the device themselves.
“People with more complex hearing loss and moderate to severe hearing loss, need to see an audiologist. But something is better than nothing for those with mild hearing loss so if people can’t afford a hearing aid and are not getting any amplification, hearables are an option and can provide a bit of support,” Dr Jayakody says.
program made them realise how important their hearing health and mental wellbeing are,” Dr Jayakody says.
“Most of the people whose results we have analysed for this part used hearables, and they decided to go ahead and purchase hearing aids because they wanted a bit more help for their hearing health.
“They said the device helped them when listening to TV or music, but they didn't feel much benefit in conversational settings when there was background noise. Things could change as we’re still doing the study but that’s the feedback we’ve had so far.”
BEHAVIOUR PROGRAM BENEFICIAL
Additionally, almost everyone who went through the behaviour activation program found it beneficial, she says.
“They had many challenges, and because of their hearing loss, there were certain activities they previously didn't want to take part in as they didn't feel comfortable,” Dr Jayakody says.
“After people completed the training provided by a psychologist trained in behaviour activation, we received many thank-yous and wonderful feedback about
how the program had helped them on their mental wellbeing journey.
“Even though we didn't see that hearables made a lot of difference, they made people realise they need to take their hearing health seriously and seek help from an audiologist, have a test and get a device tailored to their needs that can help them with their daily conversations in challenging noise backgrounds.”
These early findings of the positive influence of the behaviour program reiterate the importance of a holistic view, she adds.
“It's important when we see someone with a hearing challenge to not only fit a device to try to solve that issue but to look at how their hearing loss is affecting other areas of their life and direct them to places where they can get the support they need,” she says.
“In this day and age, we have many stresses and challenges, and if you have hearing loss, that adds to the challenges so if there are programs that can help, that is beneficial.”
Hearables can be bought over-thecounter, without a script or needing to
Ear Science chief operating officer of research, and research lead on hearing devices and implants, auditory neuroscientist, Dr David Sly, says the term hearables was coined about 10 years ago and comes from wearables.
“Hearables are basically a wireless in-ear computational device that enhances listening along with other lifestyle features,” he says. “They’ve come from the headphone market; adding hearing aid type features into earbuds makes them hearables.
“The term hearables for audiologists is primarily about amplification function for mild to moderate hearing loss but they can also include lifestyle and health biosensors."
Dr Sly says anyone who's comfortable using a smartphone can use hearables. But they don't have the fine tweaks that an audiologist can do to a hearing aid or the amplification for severe hearing loss plus battery life is much less than a hearing aid.
Many major manufacturers now have something in the hearable space including Bose, Sony and Samsung, he adds.
“They're probably taking up 15% or so of the hearing aid market,” Dr Sly says. “It's really increased because the consumer headphone companies started to add Bluetooth and microphones and once you have a microphone, amplifier, a speaker inside, a chip to do some processing and a battery, it's starting to blur the lines between consumer and medical tech.”
TECH WILL MERGE
Dr Sly predicts hearables will become smaller over time and more like hearing aids.
“I think basically the technology will merge; it will get smaller and more powerful but there's no doubt the two will physically merge,” he says. “As to who is delivering the service such as audiologists, that's a different question.
“Quite a few clinics including our Lions Hearing Clinics provide hearables, as do George & Matilda Eyecare (G&M) stores and quite a few other audiology clinics.”
To provide further context, Australian-based personalised audio technology provider Audeara Limited secured a reseller agreement in 2025 with G&M, an Australian independent optical network with more than 120 locations. G&M, which offers audiology services in some stores, is now selling Audeara Buds.
Dr David Sly and Adjunct A/Prof Elaine Wong at Ear Science Institute Australia’s Monash Innovation Laboratories.
Hearables and hearing aids at Ear Science Institute Australia.
Ear Science Institute Australia audiologist Sasha Benatar testing headphones.
Image: Ear Science Institute Australia.
Image: David Sly.
Image: Ear Science Institute Australia.
“As part of the agreement, George & Matilda Eyecare will offer Audeara’s branded assistive listening devices to customers to highlight how personalised audio solutions complement the effectiveness of tailored optical care and reinforce the importance of individualised sensory health,” Audeara said.
“George & Matilda Eyecare will initially stock the company’s recently launched Audeara Buds product, with an aim to broaden to the company’s full suite of audiology solutions for patients who may not yet require hearing aids.”
EXPANDING CLINIC SALES
Even though networks can buy in bulk, Dr Sly believes smaller independent practices should also consider selling hearables.
“It can expand their markets and sales,” he says. “For some people, like the tech savvy and younger consumers who have hearing loss, hearables might be a gateway product.
“There is a challenge that it might potentially overwhelm audiologists if there’s too much but if we just leave it to electronics retailers, which no-one is suggesting, cases might be missed.”
If audiologists sell hearables, this minimises the risk that those with more severe hearing losses will be missed and instead will be fitted. “We don’t want any delays or sitting on the fence; if someone has hearing loss, they need guidance from an audiologist,” Dr Sly says.
“This could benefit kids with conductive hearing loss, where they are experiencing reduced or muffled sounds,” Dr Sly says.
“Ear Science is excited to be working with large hearing aid companies and device companies. Our hearing devices team is working on the latest improvements to hearing diagnostics and hearing curable devices in Perth and at our new Monash Innovation Laboratories at Monash University in Melbourne.”
AUDIOLOGIST VIEWS ON HEARABLES
He does not think audiologists need to worry that hearable sales will overtake hearing aid sales if they choose to sell hearables. This is due to their visibility, shorter battery life, and being unsuitable for moderate to severe hearing loss. “Some people can also experience issues with how they fit and feel in their ears,” he adds.
Bluetooth is in most hearables and Auracast connectivity is already available in some. As more Australian venues install Auracast, their popularity will probably increase, Dr Sly adds.
Ear Science and Audeara are also collaborating on a research project to enhance the hearing of Indigenous children in remote areas in the Pilbara. They’re investigating a bone conduction hearing device for children with middle
In a recent study, Curtin University researchers Associate Professor Melanie Ferguson and Dr Ellen Bothe teamed up with Dr Bec Bennett from the National Acoustic Laboratories, to interview 12 people with hearing difficulties and six audiologists about hearables. They found adults with hearing difficulties wanted trustworthy information and support, described evaluating hearables and other devices based on compatibility with their lifestyle and needs, and expressed willingness to vary their budget according to product quality.
Audiologists reported they thought hearables were an inferior product to hearing aids, but a useful tool. They said it was not necessarily their role to assist with hearables, that hearables were a source of uncertainty, and that the provision of hearables by audiologists was not currently practical.
be an opportunity afforded by hearables to improve outcomes for people with hearing difficulties,” the researchers wrote in the International Journal of Audiology in 2025.
“Adults with hearing difficulties may have complex reasons for considering hearables and may desire a high level of clinical support in this area.
"Ongoing research into the efficacy and effectiveness of hearables is needed together with research into effective strategies to incorporate hearables into clinical practice.”
A systematic review and meta-analysis of non-medical amplification devices in adults with mild to moderate hearing loss was published in the same journal in 2025. A/Prof Ferguson, Dr Bennett and Dr Kento Nakano from ANU teamed up with UK colleagues, Dr David Maidment and Dr Maria Goodwin from Loughborough University. They evaluated 10 studies on personal sound application products (PSAPs) and four studies on smartphone amplification apps.
They found premium PSAPs appeared an effective non-medical amplification device for adults with mild-to-moderate hearing loss. Meta-analyses showed premium PSAPs improved speech intelligibility in noise performance compared to unaided, whereas basic PSAPs and smartphone apps did not.
Additionally, premium PSAPs performed better than basic hearing aids, and premium hearing aids performed better than premium and basic PSAPs, smartphone apps, and basic hearing aids. Although data could not be pooled, similar findings were found for quality of life, listening ability, cognition, feasibility, and adverse effects.
“Given the overlap in features available, it may be that this is a key consideration when drawing comparisons between devices, rather than the device being named a PSAP or hearing aid,” the researchers said. “The extent to which PSAPs are effective without audiological input remains to be determined.”
Above: Lucy Mitchell from Ear Science Institute Australia in the Pilbara.
A/Prof Melanie Ferguson (from left), Dr Bec Bennett and Dr David Maidment published a hearables study and a systematic review of non-medical amplification devices.
Images: Melanie Ferguson, Bec Bennett, David Maidment.
Image: Ear Science Institute Australia.
Trauma-informed care focuses on safety, trust, choice, collaboration, empowerment, and respect.
Trauma-informed care in audiology
MR KHALIL GAREEBOO is a clinical audiologist and trauma-informed counsellor in training. He helps people with their hearing concerns and needs as well as supporting them through their trauma journey. He also recently qualified as a Lifeline crisis support counsellor.
BY KHALIL GAREEBOO
When I first started my clinical journey, I realised the importance of counselling skills in audiology. While the fundamentals of counselling were taught at university, it was not until I started working directly with clients that I realised how counselling is a critical aspect of the profession.
While most of the audiological workload involves conducting hearing assessment, writing clinical notes and reports as well as hearing aid fitting and adjustment (depending on the workplace), there is the human aspect of our work which is undeniably present and should be addressed in a sensitive and appropriate manner.
I migrated to Australia from Mauritius after I had been looking for a rewarding profession in the allied health industry that combined people and technological skills. I discovered audiology as it was a good fit which combined these skills, and my passion for helping people.
I pursued my audiology studies at Macquarie University by completing a Bachelor of Speech, Hearing and Language Science in 2016, then a Master of Clinical Audiology.
After graduating, I moved to Mildura in regional Victoria to work at a major independent provider where I completed my clinical internship and obtained my Certificate of Clinical Practice. I later moved to Geelong to work with Amplifon during the peak of the COVID19 pandemic.
At the end of 2022 I returned to work for another independent provider in Forster, regional NSW. Although I enjoyed living regionally, I missed the benefits of living close to a major city so moved to Lithgow to work for a major adult rehabilitative hearing services provider to be nearer Sydney.
I am now undertaking a research program in public health, with a focus on hearing and vision loss, at Macquarie University under the supervision of Professor Bamini Gopinath.
BE A GOOD LISTENER
Throughout my career I have seen patients experience significant distress in their lives, notably those with sudden sensorineural hearing loss or traumatic head injury resulting in hearing loss. Simply conducting a hearing test would not be appropriate.
However, once I switched from being a clinician to being a good listener, I noticed that the clients would regain their
composure and were more receptive and grateful.
That’s when I decided to upskill and chose to enrol in mental health classes such as “accidental counselling” courses through Relationships Australia and mental health first aid classes with Mental Health First Aid Australia.
Lifeline defines “accidental counselling” as enabling people to master difficult and challenging conversations. It aims to help those who would like to safely and effectively support colleagues, family, friends and strangers who are in distress or experiencing a crisis.
This led me to undertake a Diploma of Counselling course online with TAFE NSW to expand my counselling skills. The course was highly insightful and valuable as it provided me with the soft skills required to work with a wide range of people as well as knowledge and understanding of the Australian mental health system.
I was immediately drawn to the field of
“Many audiologists already possess a basic understanding and knowledge of trauma-informed practice which can be applied in an audiological setting.”
Khalil Gareeboo Macquarie University
Image: Malik/peopleimages.com/stock.adobe.com.
Image: Khalil Gareboo.
crisis intervention and management as I found it most rewarding. It motivated me to start volunteering as a phone crisis support worker at Lifeline in 2024. This typically involves a year-long internship (depending on personal progression through the course contents, milestones, and volunteer hours) which is nationally accredited and recognised. I was taught how to respond to and manage crisis situations, including suicide prevention and domestic and family violence.
MENTAL WELL-BEING
The World Health Organization defines mental health as a state of mental well-being that allows people to manage life stresses, achieve their abilities, study and work property and thus contribute to their community. It says it is a key component of health and well-being that forms the foundation of our individual and collective capacities to make informed decisions, and develop and maintain relationships thereby influencing the world we live in.
According to Australia’s National Study of Mental Health and Wellbeing, 8.5 million Australians aged 16 to 85 years have experienced a mental disorder at some time in their life. Half meet the criteria for a lifetime mental disorder diagnosis having experienced sufficient symptoms of that disorder in the last 12 months.
Australia’s mental healthcare system is under a lot of strain due to shortages of mental health professionals and affordable services, according to Lifeline data. Additionally, people seeking mental health support often feel confused and overwhelmed trying to navigate the system.
While often overlooked in audiological practice due to a wide range of factors, clinicians should not overlook this critical aspect of their client’s well-being. This will often impact and inform the clinicians’ interactions with their clients. A holistic approach to client care will incorporate aspects of counselling such as active listening, empathising, reflecting content and feelings, as well as validating the client’s views and experiences.
However, Australian research shows many audiologists shy away from exploring clients’ mental health conditions and their effects on them during the appointment due to a lack of confidence and skills involved in discussing these issues with their clients.
Australia's standard of care in audiological practice focuses on a client-centred or family-centred approach, depending on whether the practitioner works with adults or children.
This approach acknowledges the client or family as experts in their own lives and circumstances, thereby empowering them to make informed decisions based on the information provided by the clinician
during the appointment in a collaborative and engaging manner.
This approach is valid in clinical practice as it yields positive outcomes for client-clinician interactions. But I believe it often fails to address the psycho-social dimensions of clients, especially those diagnosed with mental health conditions or experiencing crises.
SAFETY, TRUST AND CHOICE
Trauma-informed care, which is well recognised and established in the mental health field, focuses on the principles of safety, trust, choice, collaboration, empowerment, and respect. This ensures the client’s past traumatic experiences are acknowledged without re-traumatising them during the appointment.
It is based on the knowledge that many individuals living with mental health conditions have experienced trauma in their lives, its impact may be lifelong and it may affect not just the person but their emotions and relationships as well.
“Trauma” can be a lauded and often misunderstood term. It is described as an event, series of events, or set of circumstances, experienced by an individual as physically or emotionally harmful or life-threatening. It has lasting detrimental impacts on their functioning and mental, physical, social and emotional well-being for clinical purposes.
This includes adverse childhood events, domestic and sexual violence, discrimination and stigma (e.g. sexism, racism, ageism, homophobia, etc) as well as societal and structural barriers. The benefit of this approach is that it promotes recovery and healing from trauma by reaffirming the client’s strengths and resources to develop goals and strategies which are best suited for each client.
While this approach requires additional
RESOURCES
• For more information about trauma-informed practices in Australia, please visit the Blue Knot Foundation at blueknot. org.au/ or Phoenix Australia at phoenixaustralia.org/.
• If anyone is experiencing any form of crisis or issues relating to mental health, please call Lifeline (13 11 14), Beyond Blue (1300 22 4636) or SANE Australia (1800 187 263) or visit their websites, lifeline. org.au/, www.beyondblue.org.au/ or sane.org/.
• Anyone experiencing domestic and family violence can call 1800 RESPECT (1800 737 732). See also 1800respect.org.au/.
training to implement it appropriately in the appointment, many audiologists already possess a basic understanding and knowledge of trauma-informed practice which can be applied in an audiological setting. This is particularly the case for audiologists who have experienced and recovered from traumatic experiences. I strongly encourage clinicians to practise and develop those skills which will result in improved rapport and trust with clients, thereby leading to better outcomes for patients.
*References will be in the online version.
Right: Phone crisis support workers help manage suicide prevention, domestic and family violence.
Being a good listener helps clients be more receptive.
Image: Sergey/stock.adobe.com.
Image: Jordi P
Hearing Practitioner Australia is the only dedicated business-to-business publication for the nation’s hearing industry. Established out of a desire for premium, local and independent content for audiologists, audiometrists, otolaryngologists/ENTs and other Australian hearing professionals, HPA brings industry-specific reporting and analysis, in addition to the latest in news, business, products, policy, and research, plus more.
Cochlear implant milestones
Three significant milestones in Australia’s cochlear implant story were celebrated at The Royal Victorian Eye and Ear Hospital in August 2025.
rofessor Graeme Clark AC, the pioneer of the multi-channel cochlear implant, has marked his 90th birthday with a moving tribute at The Royal Victorian Eye and Ear Hospital, celebrating his legacy and
Colleagues, patients, staff, friends and family gathered in the hospital auditorium on 20 August 2025 to honour the pioneering ENT surgeon whose work has transformed the lives of people with profound hearing
The event also celebrated two other milestones: the 40th anniversary of the world’s first public cochlear implant clinic which opened at the hospital in 1985, and the hospital’s 5,000th cochlear implant recipient, Mrs Margaret Pearce, who was
lacked funds for microelectronics. With Telstra’s help and by making savings, they built the first device.
On 1 August 1978, ENT surgeon Associate Professor Brian Pyman and Prof Clark undertook the ‘make or break operation’ on Mr Rod Saunders, a former electrical linesman who had become deaf.
“The hospital was very supportive, but everyone was on tenterhooks,” Prof Clark recalled. “As I walked to my operating theatre, I passed my dear colleague Professor Gerard Crock who said, ‘Professor Clark, this is your moment of truth’, and how right he was.”
Within weeks, Saunders recognised tunes and refinements allowed him to understand words, with audiologist Ms Angela Marshall playing a key role.
Also attending were Mr Scott Smith, the first child to receive a paediatric cochlear implant in 1985 aged 10. Smith was reunited with Prof Clark and Dr Rob Webb, the surgeons who operated on him, and is still
Other special guests were Ms Sian Niame-Smith who was the first two-year-old recipient, and Hudson Stewart, aged six, who
CEO, said: “These milestones are not just numbers or dates. They represent lives changed and the enduring power of the cochlear implant and Australian
Professor Stephen O’Leary, who performed the 5,000th surgery, said the world reached its one millionth cochlear implant in 2022.
“We’ve done one in 200 worldwide – a testament to the Eye and Ear’s partnership
Professor Robert Briggs, head of the implant clinic, called it the hospital’s “jewel in the crown,” crediting audiologists, ENT surgeons and speech pathologists.
“We wouldn’t be here today without the determination and foresight of Professor
Prof Clark said patients had made a great contribution to the journey. “It’s been a privilege to work with the University of Melbourne and the Eye and Ear from 1970 and with Cochlear Limited from 1979 to create the multi-channel cochlear implant to
help hard of hearing people,” he said.
He recalled how his father’s deafness inspired him at age five to want to “fix ears.” He went on to become a doctor and after ENT training in the UK, was appointed assistant surgeon at the Eye and Ear in 1963. Three years later he read a paper on electrical stimulation of the ear that“lit the fire in the belly” to pursue research.
Though doubted by many, Prof Clark began a PhD in auditory neurophysiology at the University of Sydney before being appointed Australasia’s first professor of otolaryngology at the University of Melbourne. He built a pioneering research team to develop a working multi-channel implant and methods to test speech understanding in children.
“In this new department, we played hard, but we worked even harder often late into the night,” he said.
Funding was a struggle but $2, 000 from Melbourne Apex Club and television telethons run by Sir Reginald Ansett provided critical support.
“Without that, we would never have developed the implant,” he said.
“I sat near Angela with bated breath while she gave him the gold standard speech test and when it became clear he could understand 10% of the words it was for me a Eureka moment,” Prof Clark said. “I went into the next-door lab and burst into tears of joy; it was a very moving moment to know our work was going to be worthwhile.”
With federal backing, the team partnered with Telectronics and Cochlear to conduct clinical trials. In 1982 six patients were implanted at the Eye and Ear.
Children began receiving implants and miniaturisation of technology, with Cochlear’s engineering team, made it possible for toddlers to receive implants. Outcomes improved dramatically as children developed speech and language skills.
Today, more than 600,000 people in 180 countries have Cochlear Nucleus devices, including over 320,000 children. Prof Clark said the devices were “extremely reliable, surviving more than 20 years with 99% effectiveness.” He thanked university and hospital colleagues, engineers, audiologists, government and community donors but said none of it would have been possible without
The team who helped bring the cochlear implant to life (from left) Prof Peter Seligman, Prof Harry Minas, Dr Joe Tong, Prof Field Rickards, Prof Richard Dowell, Angela Marshall, Dr Ian Forster, Greg Cook, Prof Jim Patrick AO
Above: Prof Robert Briggs (from left), Scott Smith, Hudson Stewart, Prof Graeme Clark, his wife Margaret Clark, and Margaret Pearce.
A bright future
Macquarie University Hearing’s inaugural Hearing Research Symposium led by early and mid-career researchers from across Australia was a great success, drawing more than 100 online attendees.
The strength and impact of hearing research in Australia was highlighted at Macquarie University Hearing’s first Hearing Research Symposium.
Patients, practitioners, researchers, industry and association representatives tuned in to hear local researchers update on studies and programs which ranged from helping audiologists assist patients with hearing loss to improve their mental health and wellbeing, to delivering gene therapy via cochlear implant electrodes.
Ms Michele Nealon, Macquarie University Hearing coordinator, and the Macquarie University Hearing Grassroots Network, organised the event on 25 August 2025. Nealon said it showcased the talent and passion of Australia’s next generation of hearing researchers. Chair was Dr Heivet Hernandez-Perez, Macquarie University postdoctoral research fellow.
AIMER SUPPORTS WELLBEING
Dr Bec Bennett, principal research audiologist from the National Acoustic Laboratories, explained how an Australian-developed world first program to help audiologists better support the social and emotional wellbeing needs of adults with hearing loss is going global.
The AIMER (Ask, Inform, Manage, Encourage, Refer) program is already used
successfully in Australia’s Lions Hearing Clinics, Audika and several independent audiology clinics across Australia.
"Groups overseas are now adopting the AIMER framework," Dr Bennett said.
She said people with hearing loss were at high risk of social isolation, loneliness, anxiety and depression. Her 2019 survey of hearing practitioners found approximately half focused only on audiological issues, overlooking the social and emotional wellbeing concerns raised by clients.
“Awareness of the need for this support was high,” she said, “but many practitioners felt they lacked the skills and confidence to provide holistic care.”
The AIMER framework was developed to bridge this gap, offering tools to help practitioners address clients’ broader needs, she said.
A recent trial showed it to be highly effective, enabling clinicians to more frequently discuss and support social and emotional wellbeing during appointments. More information about AIMER and its resources is available at youtube.com/@ DrBecBennett.
DEVELOPING A NEW COCHLEAR IMPLANT ELECTRODE COATING
Dr Jacqueline Ogier is a postdoctoral research fellow at the University of Melbourne who focuses on molecular
biology in the inner ear. She described the early stages of developing a novel bioactive coating for cochlear implant electrodes.
This work built on her PhD at the Murdoch Children’s Research Institute where she focused on oxotoxicity and identified that apoptosis signal-regulating kinase 1 (ASK1) is an important mediator of sensory hair cell death.
Around the same time, several research groups also found ASK1 was a molecular target for preventing inflammation and
Above: Speakers were (from left, top) Dr Fadwa Alnafjan, Dr Bec Bennett, Dr Jeremy Pinyon. (From left, bottom) Dr Emma Laird, Dr Diana Tang, Dr Jackie Ogier.
Images: Macquarie University Hearing.
Event chair was Dr Heivet HernandezPerez.
Image: Heivet Hernandez-Perez.
fibrosis in models of kidney, liver and cardiac disease. As a result, Selonsertib, an ASK1 inhibitor, was tested in phase one to three human clinical trials.
With this in mind, Dr Ogier has been investigating if Selonsertib can be used to prevent inner ear hair cell death, inflammation, and fibrosis post cochlear implantation to improve hearing outcomes.
She described the process of evaluating polymer coatings and their drug elution profiles, plus her subsequent proteomics that evaluate the molecular effect of the new electrode coating.
“The interface between cochlear implants and electrodes is the next step of safe and effective interventions,” she said.
GENE THERAPY VIA COCHLEAR IMPLANTS
Neuroscientist, Dr Jeremy Pinyon described his work of the past 15 years with co-investigators on the cochlear implant neurotrophin gene therapy clinical trial. The research is investigating improving the quality of hearing, particularly tone, delivered through cochlear implants.
Dr Pinyon is a lecturer at the University of Sydney’s School of Medical Sciences where he heads the Neuroregenerative Gene Therapy group.
He co-developed close-field electroporation – gene electrotransfer using cochlear implant electrodes to deliver therapeutic genes into the inner ear.
“We’re working to close the neural gap by introducing nerve growth factors (neurotrophins) into the cochlea,” he said. “This non-viral gene therapy creates an electric current to drive transfer of the genes.”
The growth factors create an augmented and improved interface, he said.
The team found delivering these growth factors during cochlear implant surgery stimulated auditory nerve fibres in the cochlea to regrow towards cochlear implant electrodes in animal studies.
Additionally, studies in deaf guinea pigs showed enhanced performance of cochlear implants when the growth factors stimulated auditory nerve fibres to re-grow towards the electrode array, Dr Pinyon said.
A trial in humans is continuing.
FEWER SAFETY CONCERNS
Lead audiologist in the trial hosted by the Translational Neuroscience Facility at UNSW, Dr Fadwa Alnafjan, a Macquarie University lecturer and research audiologist, said that during the gene electrotransfer, brief electrical pulses helped cells take up the therapeutic DNA.
“One advantage of this method (of delivery) is that there are fewer safety and research barriers of provoking the immune system,” she said.” It offers a promising clinical way of delivering genes and the therapy is targeted exactly where it’s needed.”
In 2020 a trial involved 24 adults with profound hearing loss, 16 who received the therapy and eight controls. One year follow-up revealed no adverse reactions, Dr Alnafjan said.
“ There were no safety flags, including recoding impedance, which is a marker for inflammation,” she said. “Steep and rapid improvements suggested the gene therapy had driven accelerated recovery of functional hearing.”
Further follow-up indicated encouraging, early evidence of the pace and quality of auditory nerve regeneration and improved hearing performance rehabilitation post implantation. “There were stronger and faster neural responses in the treated group than controls, and faster and bigger differences were maintained post operatively,” she said,
SELF-GUIDED MENTAL HEALTH SUPPORT
Audiologist Dr Emma Laird, La Trobe University senior audiology lecturer, discussed Luminear, a Melbourne innovation to provide mental health support for those with hearing loss through a personalised self-guided digital program. She worked on the program with Soundfair and The University of Melbourne.
“People wanted a solution in between what
psychologists and audiologists were offering,” she said. “We’ve just started analysing preliminary results of our randomised controlled trial in 105 participants.”
Participants were mainly female, aged in their late 50s and early 60s, most used hearing aids and had had hearing loss for an average 24 to 26 years. Half were given three months’ access to the program.
Dr Laird said the dropout rate and lack of improvement in wellbeing or quality of life six months post intervention were possibly due to the wrong demographic being targeted - participants who had had hearing loss for many years and may have learnt their own coping strategies. Aiming for those within ten years of starting their hearing loss journey might deliver different results.
DUAL SENSORY IMPAIRMENT
Macquarie University Hearing postdoctoral research fellow, Dr Diana Tang, discussed her research on wellbeing in adults with dual sensory impairment (DSI) and their communication partners. “One in four people over 80 have dual sensory vision and hearing impairments such as age-related macular degeneration and hearing loss,” she said. “They have two to three times higher incidence of anxiety and depression than those without dual sensory impairment.”
Dr Tang studied barriers to wellbeing in people with DSI over 65 and their communication partners. She is working on a project to co-design a wellbeing program with Macquarie University and University of Sydney colleagues, older people with DSI from age-related causes and service providers.
She is also joint organiser of the 2025 National Dual Sensory Impairment –Deafblindness Conference in Sydney from 27 to 28 November. It brings together people and families living with DSI – deafblindnes plus professionals, practitioners, researchers and organisations. Visit dsiproject.org.
Dr Jeremy Pinyon’s slide showing development of a gene delivery probe via a cochlear implant. Image adapted from Pinyon et al, Advanced Science, 14 June 2024. DOI: 202401392.
Image: Jeremy Pinyuon.
Joint event organiser, Macquarie University Hearing coordinator, Michele Nealon.
Image: Michele Nealon.
Flexible CPD in online event
Audiology Australia’s upcoming online conference will feature innovation, research and information that audiologists can put into practice.
The Audiology Australia (AudA) Online Conference on 23 and 24 October 2025 offers two dynamic half-days of learning, connection, and inspiration.
It will enable delegates to upskill and gain continuing professional development points from their home or clinic, offering two four-hour sessions for those seeking to fit CPD around the challenges of a busy life.
Ms Leanne Emerson, AudA CEO, said: “This event is part of our continuing commitment to offer flexible, practical, contemporary CPD to members and Australian audiologists that works around life and its challenges in and beyond the clinic.
“We’ve created a virtual conference that lightens the load without compromising on quality so attendees can fit their learning to their schedule while still gaining insight and knowledge ready to use in the clinic.”
SPEAKERS AND TOPICS
The event goes from 3:30pm to 8pm AEDT on Thursday 23 October, and 11am to 3:30pm AEDT on Friday 24 October. Registration gives full access to every session across both days plus the flexibility to catch up later. All content will be available on demand until 18 January 2026 to watch, rewatch, and claim CPD points when suited. Up to eight hours of CPD is available. For each hour that AudA full members complete, they will obtain one CPD point in category 1.2. Delegates need to complete a quiz or reflection to be eligible for CPD points.
Three sessions meet Certified Advanced Paediatric Audiologist (CAPA) CPD requirements to maintain certification. They are the ANCHOR, EarGenie and Flying Colours sessions which offer 2.5 CPD points in total.
The ANCHOR presentation will discuss
collecting, connecting and transforming child hearing health information into a learning health system; the EarGenie talk updates on an upcoming innovation to help audiologists fast-track early intervention for hearing loss; and Flying Colours is a one-stop resource for families as they navigate a new world with a DHH child.
AudA said delegates could expect a packed program from expert speakers offering sessions ranging from brain imaging for tinnitus to hearing health data for children, real world story sharing, and home based audiology.
The conference is open to AudA members and student members as well as non-members.
People can register via the events calendar at audiology.asn.au or audiology.eventsair. com/audaonline25.
A/PROF MEHRNAZ SHOUSHTARIAN, BIONICS INSTITUTE
A/Prof Shoushtarian will discuss objective assessment of tinnitus to identify presence, severity and subtypes based on brain imaging and underlying neural activity. Currently clinical assessment uses subjective feedback from individuals, which is not always reliable and is prone to placebo effects. Her team has shown sensitivity of a non-invasive brain imaging technique, functional near-infrared spectroscopy, to detect tinnitus presence and severity. Such measures are a critical step in developing new treatments and monitoring treatment progress.
DR BARBRA TIMMER, THE UNIVERSITY OF QUEENSLAND
Dr Timmer will give an update on National Railway Standards and what new hearing guidelines mean for audiologists. Recent updates to the National Standard for Health Assessment of Rail Safety Workers have brought notable changes to the audiological guidelines used for assessing workers in safety-critical rail roles. Dr Timmer will outline the key revisions, explain their implications for audiologists, and highlight how these updates affect clinical testing and reporting requirements.
Delegates can attend the online conference from the comfort of their own home or office.
Image: Fizkes/Shutterstock.
SPEAKERS AND TOPICS
ADJ/PROF ROB EIKELBOOM, JESSICA YIANNOS & LUCY MITCHELL, EAR SCIENCE INSTITUTE AUSTRALIA
The trio will discuss ear and hearing health in remote communities in the Pilbara including how data is informing service improvements. They will detail how a multidisciplinary team will examine the prevalence and incidence of hearing loss and ear disease of Aboriginal children in five East Pilbara communities over 10 years. Multiple data sources will be combined and analysed to inform service provision and improve the hearing health of Indigenous children in the region.
PROFESSOR COLETTE MCKAY, BIONICS INSTITUTE
Prof McKay will give an update on EarGenie, a brain imaging system that aims to help audiologists fast-track early intervention for hearing loss. The device aims to remove roadblocks that delay early intervention for hearing loss particularly auditory neuropathy. Her team led development of fNIRS technology for clinical applications in paediatric audiology and built the clinician and baby-friendly system which includes a headband that connects to a laptop via Bluetooth. A commercial version will be manufactured in the next 12 months with eventual widespread availability in clinics.
DR KATIE EKBERG, FLINDERS UNIVERSITY
Dr Ekberg will reveal a new model for understanding stigma related to hearing loss. She will provide an overview of findings from a large, multi-method study that investigated how stigma is experienced by adults with acquired hearing loss and their families, how they manage it in everyday life, and how these experiences relate to the decision to try hearing aids and to wear them in the long-term. She will discuss implications for audiology clinical practice.
PROFESSOR KEVIN MUNRO, UNIVERSITY OF MANCHESTER
DIY audiology at home is the topic of Prof Munro’s talk. Adults are interested in conducting self-administered hearing tests and trying fit-at-home hearing aids. He will investigate if these could transform how services are delivered. His presentation will share findings from a UK survey of more than 2,000 adults, exploring attitudes to at-home hearing solutions, what people see as benefits and barriers, how preferences shift across age groups, and what this could mean for the future of sustainable, accessible hearing care.
A/PROF VALERIE SUNG, THE ROYAL CHILDREN’S HOSPITAL
A/Prof Sung will discuss the Australian National Child Hearing Health Outcomes Registry (ANCHOR) which aims to collect and connect child hearing health information to drive service improvements and create a pipeline for research discoveries. Its vision is to give all deaf and hard of hearing children the best opportunities to reach their full potential and live healthy, fulfilled lives. She will focus on phase one which aims to establish prerequisites of a national database.
SARAH BRENNAN, TAMARA TRINDER-SCACCO & STACEY JOHNSON, DEAF CHILDREN AUSTRALIA
Flying Colours is a one-stop resource for families as they navigate a new world with a DHH child. The presentation will give an overview of what the website covers and recent initiatives that have resonated w ith certain cohorts. The online resource provides information, stories from parents with a lived experience and DHH young people about growing up deaf, research articles, links, and a service finder. Trinder-Scacco and Johnson will share their lived experience of navigating their world with a DHH child.
DR RACHAEL TAYLOR, THE UNIVERSITY OF AUCKLAND
Dr Taylor will present on higher order vestibular processing and impaired vestibular perception as a hidden cause of imbalance. Increasing evidence suggests some balance problems could be due to impaired perception of vestibular input. Studies have identified a sub-set of patients with “vestibular neglect” or “vestibular agnosia” – normal peripheral vestibular function but increased thresholds for perception of linear and angular motion. She will review knowledge on mechanisms and patient characteristics underlying poor vestibular perception, and its functional implications.
DR GARGI PATHAK, GENETIC HEALTH WESTERN AUSTRALIA
Dr Pathak will discuss genetic conditions and hearing health. Genetic hearing loss exhibits considerable diversity, with numerous genes harbouring mutations which can cause syndromic or non-syndromic hearing loss. Molecular diagnosis is expected to expand further, encompassing more mutations and genes. There are Medicare rebates for genomic testing and copy number variant analysis of some genes known to be causative or likely causative of childhood hearing loss. Genetic analysis for hearing loss is mainly used for diagnosis and treatment.
WEAN STEROIDS TO AVOID AN ADRENAL CRISIS
Intra or transtympanic corticosteroids can result in significant systemic absorption so consider weaning them in a similar way to oral prednisone to avoid an adrenal crisis, advises nephrologist Professor SIMON ROGER.
CAN MARKEDLY SUPPRESS THE BODY’S CORTISOL PRODUCTION.”
PROFESSOR SIMON ROGER
Sensorineural deafness or hearing loss is caused by damage to the cochlea or the auditory nerve. The onset can be sudden or gradual. The hearing loss can occur on one side or both. Symptoms can be very debilitating. It is the commonest type of permanent hearing loss.
The hearing loss can relate to a range of issues including a concurrent illness including infections, loud noise, diabetes, trauma to the head and some medications such as gentamycin and cisplatin.
The use of corticosteroids can be controversial as discussed in both a Cochrane review and clinical practice guidelines. The evidence has been described as low or very low certainty. These can be administered orally, intra or transtympanic, or a combination of both as primary therapy.
Oral corticosteroids, eg prednisone or dexamethasone, are used in a wide range of medical conditions whether it be treating autoimmune diseases such as systemic lupus erythematosus or rheumatoid arthritis, vasculitis or exacerbation of airways disease.
AVOIDING ADDISONIAN CRISIS
It is well recognised by the medical profession that oral steroid dosages need to be weaned over a period of time (depending on the initial dose and duration of therapy) to allow the adrenal glands, which produce endogenous steroid (cortisol) to recover after a period of suppression. Failure to do that can result in an Addisonian crisis, also known as an adrenal crisis.
The steroids can also be administered directly into the middle ear, using drops via a grommet or transtympanic injection 3x/week or on alternate days. Relatively large doses of steroids are administered via this route.
The transtympanic method is typically but probably incorrectly prescribed to reduce absorption in patients with diabetes mellitus, unstable hypertension, propensity to gastric ulcer disease, glaucoma or prior psychiatric reactions (steroid psychoses), who may not be able to receive corticosteroids orally. There is a propensity for
the absorption, either through the middle ear or from drainage down the eustachian tube, to be swallowed and absorbed in the stomach.
PERSONAL EXPERIENCE
I have worked as a renal physician for more than 30 years and have a history of type I diabetes dating back 45 years. During 2023-2024, I suffered two episodes of sensorineural hearing loss, affecting both ears.
Initial management was oral prednisone and transtympanic steroid injections. The second episode, rather than injections, involved the insertion of a grommet and administration of dexamethasone drops.
Dexamethasone is a more concentrated steroid preparation with 0.5mL (24mg/mL) on alternate days for two weeks, equating to 75mg prednisone. This followed four weeks of oral prednisone 50mg/day, titrated over that time period.
Not surprisingly, the systemic and intra-tympanic steroids caused significant side effects. These included increasing insulin dosages by 250%, insomnia, anger management issues and tremor.
The sudden withdrawal of the intratympanic steroids resulted in an Addisonian crisis with a blood pressure of 90/72mmHg. A random cortisol taken at
the time came back very low at 44nmol/L; normal range is 130-650nmol/L. The hypotension responded within an hour to oral prednisone 5mg.
TEACHING POINTS
It is well recognised that oral prednisone dosages need to be titrated over time. However, it is not well recognised that intra or transtympanic corticosteroids, as they are absorbed, can markedly suppress the body’s production of cortisol. Therefore, the prescribing otolaryngologist should be aware of this phenomenon and consider weaning that route of administration of corticosteroids, in the same way that oral dosages are titrated downwards.
Appropriate discussion needs to occur between the otolaryngologist and the patient and may also involve the general practitioner to help with supervision of the process.
*Prof Roger and Dr Thomas Kertesz from the Sydney Adult and Children’s Ear Nose and Throat Surgery Centre, Randwick, first wrote a letter to the editor of the Australian Journal of Otolaryngology in May outlining this case. It aimed to create awareness among ENT specialists about the importance of titrating down transtympanic corticosteroids, rather than abrupt cessation.
ABOUT THE AUTHOR: Prof Simon D Roger MD FRACP was director of Gosford Hospital’s Department of Renal Medicine and is current director of Renal Research Gosford NSW. He has more than 30 years of clinical experience and is principal investigator for more than 100 clinical drug trials.
Corticosteroids such as prednisone are used in a wide range of medical conditions.
Image: Simon Roger.
OCCUPATIONAL HEARING SCREENING
Occupational hearing screening is a vital shield against noise-induced hearing loss, says audiologist DR ANNEMAREE DALEY.
“OCCUPATIONAL HEARING SCREENING FORMS A LEGALLY MANDATED, EVIDENCEBASED CORNERSTONE OF NOISE RISK MANAGEMENT IN AUSTRALIAN WORKPLACES.”
In today’s bustling work environment, many employees are routinely exposed to high noise levels. While the ambient sounds of machinery or construction might be part and parcel of their daily grind, a dangerous, insidious threat looms: noise-induced hearing loss (NIHL).
To combat this, Australia has made strides in instituting robust occupational hearing screening programs aimed at safeguarding workers' auditory health. But what exactly is occupational hearing screening, and why is it essential?
UNDERSTANDING SCREENING
Occupational hearing screening, or audiometric testing, is a systematic approach to measuring an employee’s hearing thresholds. By assessing thresholds, specialists can identify declines in hearing ability over time, particularly those resulting from workplace noise exposure.
The most common method is pure-tone audiometry, which helps establish a worker’s baseline hearing level on starting a job with noise-related risks. Periodic monitoring then catches threshold shifts before they escalate into irreversible damage.
The goals of screening are clear:
- Establish a reference test to create a baseline hearing profile when employees initiate work in noisy conditions.
- Conduct regular monitoring assessments to identify early signs of hearing deterioration.
- Gather data to evaluate the efficacy of engineering, administrative, or protective measures implemented to manage noise exposure.
WHY PRIORITISE SCREENING?
1. Prevention of NIHL: Hearing impairment often develops gradually and, regrettably, can
become irreversible. Implementing early detection practices empowers employers to intervene by reducing noise exposure or enhancing protective measures before permanent damage occurs.
2. Legal and regulatory compliance: Employers in Australia must adhere to Work Health and Safety (WHS) laws, which require them to proactively manage noise risks. Certain conditions necessitate audiometric testing, and non-compliance brings significant penalties and potential exposure to workers’ compensation claims.
3. Worker welfare and safety: Ramifications of untreated hearing loss extend beyond the individual; they can deter communication, compromise mental health, and diminish workplace safety, especially when employees need to hear warnings for imminent dangers. Proactive hearing screening ensures timely support for affected workers.
4. Financial incentives: Preventing hearing loss doesn’t just protect employees; it also significantly cuts costs. By mitigating the risks and enhancing workplace safety, employers can reduce expenses related to workers’ compensation claims, lost productivity, and potential healthcare costs.
5. Effective risk management and monitoring: Regular hearing assessments allow employers to monitor auditory health trends, assessing if noise controls (engineering solutions, administrative strategies, personal protective equipment) remain effective. This ongoing process encourages continual improvement in workplace safety standards.
REGULATORY FRAMEWORK
The foundation of Australia’s approach lies in its WHS laws. These regulations, while uniformly adopted, have varying implementation dates across states and territories. Key standards include a noise exposure standard set at an average of 85 dB(A) over an eight-hour shift, and compliance with the Australian Standard AS/NZS 1269.4:2014, outlining best practices for audiometric testing. Model WHS Regulations, specifically Regulation 58, say employers must conduct
audiometric testing for workers frequently required to use personal hearing protection due to excessive noise exposure. Essential elements of this regulation include:
• A baseline hearing test within three months of an employee starting work in a noisy environment.
• Follow-up tests at least every two years thereafter, with employers responsible for organising and paying for assessments.
STATE VARIATIONS
Each state and territory integrates these regulations in ways suited to their unique labour environments. For instance:
• NSW mandates that from 1 January 2024, employers must conduct hearing tests for workers regularly using hearing protection, with existing workers required to be tested by 1 January 2026.
• WA aligns closely with these requirements but also mandates test results be maintained in records for at least two years.
• Queensland has similar stipulations, with new regulations taking effect by 29 July 2025, reinforcing the importance of sound occupational health practices.
Occupational hearing screening is not optional; it forms a legally mandated, evidence-based cornerstone of noise risk management in Australian workplaces. It helps protect workers’ health and safety, supports legal compliance, reduces long-term costs, and helps maintain productivity.
Because rules vary slightly by state/territory, it's essential for each employer to check with their WHS regulator, refer to AS/NZS standards, and implement a robust hearing conservation program.
For businesses seeking expertise in employee occupational hearing screening, the Australasian College of Audiometry offers an Occupational Audiometry Course comprising a two-day face-to-face workshop and online learning module. It provides skills and knowledge in line with AS/ NZS 1269.4:2014 Occupational Noise Management - Auditory Assessment Standards. See auca.edu.au/
Below: A baseline hearing test should be done within three months of starting work in a noisy environment.
Image: Peakstock/Shutterstock.
DR ANNEMAREE DALEY
ABOUT THE AUTHOR: Dr Annemaree Daley is an educator with the Australasian College of Audiometry.
Image: Annemaree Daley.
NEW LAWS THAT SMALL BUSINESS SHOULD KNOW
LYNDON BURKE explains staff can now ignore their employer’s calls after hours, and discusses other new laws enacted this year that small businesses including audiology clinics need to know.
“AUDIOLOGY CLINICS MUST BE CONSCIOUS OF THE RIGHT TO DISCONNECT.”
As of 26 August 2025, Australian small business employees have the legal right to ignore work calls, emails and messages outside their contracted hours – unless the contact is deemed 'reasonable.' Similar rights have been available to employees in large organisations since 26 August 2024.
The new disconnect laws are embedded in the Health Professionals and Support Services Award 2020 and the Fair Work Act 2009 (Cth). Audiology clinics must be conscious of the right to disconnect. Urgent rostering changes or other urgent requests may give rise to reasonable requests.
The right to disconnect is already making headlines, with Queensland school teacher Ms Michelle Martin suing her former employer Cairns Rudolf Steiner School for nearly $800,000 in damages over after-hours contact.
Cases like this show the law isn’t just a symbolic change – there’s real legal and financial risk for employers who get it wrong. If you haven’t updated your policies and trained your managers, you could be next.
Below: The disconnect law means employees have the legal right to ignore work calls, emails and messages outside their contracted hours.
WHY IT MATTERS FOR SMALL BUSINESS
While big corporates often have human resources teams to handle compliance, smaller operators face the same legal obligations with fewer resources to manage the risks.
The law doesn’t care if you have five employees or 5,000. If you breach these new rules, the penalties and reputational damage can be devastating.
Proactive compliance isn’t just about avoiding fines – it’s also good for business. Getting this right builds trust with your staff, reduces turnover and protects your brand. It’s not just a legal requirement; it’s a competitive advantage.
If employers take action against employees who exercise the right to disconnect, they could be exposed to claims for damages, penalties and potentially penalties for award breaches.
OTHER CHANGES SMEs SHOULD KNOW
The right to disconnect is just one of several major employment law changes in 2025 that could catch small business owners off guard. These include:
1. Wage theft is now a criminal offence, from 1 January 2025
Intentionally underpaying staff is now a crime, carrying potential jail time for individuals and multi-million-dollar fines for companies.
This isn’t just about dodgy operators. Even payroll mistakes can lead to significant penalties – and in some cases, criminal liability.
2. Superannuation increase to 12%, from 1 July 2025
The compulsory super guarantee rate has recently risen from 11.5% to 12%, increasing payroll costs for all employers.
Small business owners need to factor this into their budgets now. It’s not just an extra 0.5% — it can have a real cashflow impact, especially if you have a large casual workforce.
3. Award classification and pay rate updates, from 1 January 2025
Modern award changes have introduced new entry-level classifications and pay rates across multiple sectors.
The Health Professionals and Support Services Award 2020 is not affected by the changes that came into effect from January 2025.
Nevertheless, audiology businesses must still be mindful that audiologists are health professionals and when a graduate starts, their minimum pay rates increase on
an annual basis (clause 17 of the Award). The same minimum pay progression applies to support services employees where there is more than one pay point in the relevant classification (clause 16 of the Award).
Misclassification is one of the biggest compliance risks. Even a minor error can trigger back-pay obligations and fines.
HOW SMEs CAN STAY COMPLIANT
Small and medium enterprises (SMEs) should take these immediate steps if they have not already done so:
1. Review their policies and contracts – especially regarding after-hours contact.
2. Audit their payroll and timekeeping systems – to ensure correct pay rates and entitlements.
3. Update their budgets – to account for higher super contributions from July.
4. Train managers and supervisors – on the new Right to Disconnect obligations and respectful communication.
5. Seek advice early – before the Fair Work Ombudsman, Fair Work Commission, a Federal Court or a tribunal gets involved.
A quick review with an employment lawyer now can save thousands in fines and legal costs later. The days of informal, ‘she’ll be right’ approaches to HR are over.
Burke Mangan Lawyers has published practical explainers for employers and employees on navigating the right to disconnect including a checklist for employers about the right to disconnect. These can be viewed on its website at bm-lawyers.au.
More information about the right to disconnect can also be found on the Fair Work Ombudsman’s website at fairwork.gov.au.
LYNDON BURKE
DEAFNESS, HEARING LOSS, AND MENTAL HEALTH
A discussion on breaking down barriers to care, system challenges, lived experiences, and the path forward.
hard of hearing, and have mental health care concerns experience the healthcare system.
I’ll mostly use “hearing loss” but want to respectfully acknowledge that this term doesn’t capture everyone’s unique identity or diverse experiences. Everyone has the right to self-identify.
Our research wasn’t just data collecting, it was about stories and voices of the communities of those with hearing loss, so we can uplift and amplify them to support systemic positive change.
Mental health care is already hard to access, but for people with hearing loss, barriers are often higher and more complex because of unique communication needs and distinct mental health challenges.
When hearing loss meets mental health, the risks of isolation and miscommunication multiply — and the system isn’t keeping up.
MENTAL HEALTH IMPACTS OF OVERLOOKED HEARING LOSS
In our research with people with hearing loss, more than half said they deal with ongoing stress. Nearly half reported feeling socially isolated. And more than 40% said they experience anxiety. These numbers are sobering but not surprising.
About 3.6 million Australians live with hearing loss. While national data linking hearing loss and mental health is limited, evidence consistently suggests higher rates of mental health issues, such as anxiety, depression, loneliness,
and social withdrawal in this group compared to the general population. Why? Because navigating a world designed for hearing people brings ongoing communication challenges and mental fatigue.
When people seek help, these challenges often worsen. Health providers may speak too quickly, avoid eye contact, or don’t offer accessibility options.
Hearing fatigue and the effort needed to understand is often overlooked. Instead of checking that communication was clear and needs were met, assumptions are made — leaving people feeling unsupported. Simple actions like providing takeaway notes, assistive technology, or gentle follow up questions, could make the difference.
ONE SIZE NEVER FITS ALL
Hearing loss isn’t just a physical issue that can always or entirely be fixed with a device. It’s about identity, energy, communication, and connection. When those things are missing, mental health suffers. No two people experience hearing loss the same way. Some identify as culturally Deaf and use Auslan For them, being Deaf is a distinct culture, not disability. Others lose hearing later and grieve what’s gone. Some speak, some sign, some both some neither. Yet, our health system rarely reflects this diversity. Instead, it offers one-size-fits-all care that leaves many feeling unsupported. What people want is simple: support that meets them where they are — not where the system assumes they should be.
COMMUNICATION BARRIERS ARE OBSTACLES TO CARE
Practitioners need to develop competencies in genuinely inclusive communication which meets the person’s communication needs in a person-centred way. It could be captions, it could be Auslan or something else. Otherwise, communication barriers can lead to insufficient support. It may mean delayed care, frustration, and sometimes people just stop trying. Genuine support might be insufficient when practitioners don’t speak the language people need — literally, figuratively, and culturally.
HOW THE SYSTEM CAN CHANGE
Our research recommends:
• Making communication accessible everywhere — captions, visual aids, plain language, and always ask how someone prefers to communicate.
• Integrating hearing and mental health care — build shared care plans and coordinated, person-centred services.
• Training health practitioners in Deaf culture, inclusive communication, and mental health impacts of hearing loss.
• Raising public awareness to reduce stigma and build understanding about hearing loss and mental health.
• Creating flexible, person-led systems;, funding Deaf-led services, embracing inclusive technology. Codesign changes with hearing loss communities. If you’re a health practitioner, or are supporting a person with hearing loss, and want to know what next, start with asking them: “How do you prefer to communicate?”
Make space for people to share their world. Don’t assume you know. Be curious. Be respectful. Communication isn’t just talking — it’s connection.
You don’t have to get it perfect. But you do have to try because when mental health care ignores hearing health, it’s not holistic and misses the full picture — leaving behind people unsupported. We should do better. And we can.
Name: Jane Lee
Health qualifications: Masters of Bioethics, Masters of Public Health, Bachelor of Science, Social Science Affiliations: Deafness Forum Australia
Location: Canberra, Australia.
“WHEN HEARING LOSS MEETS MENTAL HEALTH, THE RISKS OF ISOLATION AND MISCOMMUNICATION MULTIPLY.”
Above: The research found nearly half reported feeling socially isolated.
Image: Jane Lee.
People on the move
REBECCA GAY LEADS WSA WHOLESALE ANZ
Ms Rebecca Gay is WS Audiology's new managing director of Wholesale, Australia and New Zealand, effective 1 October 2025. WSA said her appointment marked a significant step in its investment in leadership excellence and commitment to delivering value to wholesale customers. With more than two decades of experience in the hearing care industry, Gay brings a unique blend of clinical expertise and strategic acumen to the role. She has a Master of Clinical Audiology from Macquarie University and degrees in science and psychology from the University of Sydney. Gay will report to WSA’s APAC president and join the APAC leadership team.
BOB COWAN JOINS THE SHEPHERD CENTRE BOARD
The Shepherd Centre has appointed Professor Robert (Bob) Cowan to its board of directors. A global leader in audiology and hearing sciences, Prof Cowan is director of HEARnet Clinical Studies, a principal research fellow at The University of Melbourne, and has honorary appointments at The Royal Victorian Eye and Ear Hospital. He has had senior roles with Audiology Australia and the International Society of Audiology, and his contributions have been recognised with awards and international fellowships. The Shepherd Centre said Prof Cowan’s expertise and lifelong commitment to improving outcomes for people with hearing loss would be invaluable.
NEW EYE AND EAR DIRECTOR OF MEDICAL SERVICES
Dr Nathan Vos is the new director of medical services at The Royal Victorian Eye and Ear Hospital. He gained his Bachelor of Medicine and Bachelor of Surgery, Medicine from the University of Tasmania, before working for the Department of Health in Tasmania. Dr Vos later worked for Monash Health and Cabrini Health in Melbourne. He has experience in medical administration and is a Fellow of the Royal Australasian College of Medical Administrators. He also has a dual Master’s in Public Health and Health Leadership and Management. Dr Vos has been supporting the hospital as its medical administration fellow since the start of 2025.
Mrs Charlen Lavoie has joined The Audiology Place independent audiology practice in Forestville, NSW. Owner Dr Signe Steers said their professional paths had been intertwined for more than 20 years and they had now joined forces again. Lavoie has a Bachelor Science du Langage from Universite du Quebec a Montreal, a Master Science de la Sante (Audiology) from Universite d’ Ottawa and specialises in full scope audiology, with a particular interest in complex diagnostics. Dr Steers said with their long-standing professional relationship built on trust, experience, and shared values, their collaboration brought strength and continuity to the practice.
AG BELL ACADEMY APPOINTS TRUDY SMITH
The AG Bell Academy for Listening and Spoken Language in Washington DC has appointed Australian teacher of the deaf Ms Trudy Smith to its board of directors. Smith has taught since 1988 and is NextSense Institute’s Continuing Professional Education manager and adjunct lecturer at Macquarie University. The academy is an independent subsidiary of the Alexander Graham Bell Association for the Deaf and Hard of Hearing, and global accrediting body for certified Listening and Spoken Language Specialists in early intervention or education. Smith will remain in her NextSense role and attend board meetings remotely apart from one in-person visit to the US annually.
ERIC BERNARD IS THE NEW CEO FOR SONOVA
Mr Eric Bernard is the new Sonova CEO, effective 15 September 2025. Sonova Holding AG announced on 15 September that he had officially stepped into the role. Bernard joined the group on 1 July 2025, and succeeds Mr Arnd Kaldowsk who had been in the role since 2018. Bernard previously worked for the Essilor Group for 20 years including being its ANZ CEO from October 2000 to June 2005. He also worked for Nikkon-Essilor, was chairman of the board for hear.com, and worked for WS Audiology in Denmark including being its group president and CEO for nearly five years.
CHARLEN LAVOIE JOINS THE AUDIOLOGY PLACE
Image: The
Image: Charlen Lavoie.
Image: Sonova and Geri Krischker.
EVENTS CALENDAR
To list an event in our calendar please email helen.carter@primecreative.com.au
OCTOBER 2025
AUDIOLOGY AUSTRALIA ONLINE CONFERENCE
Melbourne, Australia 23-24 October audiology.eventsair.com/audaonline25
VICTORIAN TEMPORAL BONE SURGICAL COURSE
Melbourne, Australia 23-24 October asohns.org.au
LIVE ENT SURGERY EVENT Melbourne, Australia 24 October events.humanitix.com/live-ent-surgery-event
ANZRS 25 CONFERENCE Queenstown, New Zealand 24-25 October asohns.org.au
ITINERANT TEACHER OF THE DEAF CONFERENCE 2025
Sydney, Australia 31 October nextsense.org.au
NOVEMBER 2025
FRONTIERS 2025
Hobart, Australia
13-15 November thefrontiersconference.org
ST VINCENT’S 40TH TEMPORAL BONE DISSECTION COURSE
Sydney, Australia 14-16 November asohns.org.au
AUDIOLOGY AUSTRALIA WA CONFERENCE
Perth, Australia 28 November audiology.eventsair.com/wa-conference-25
BRITISH ACADEMY OF AUDIOLOGY ANNUAL CONFERENCE 2025
Telford, Shropshire, England 20-21 November baaudiology.org
ASHA 2025
Washington DC, US 20-22 November asha.org/events/
DUAL SENSORY IMPAIRMENT DEAFBLINDNESS CONFERENCE
Sydney, Australia 27-28 November dsiproject.org
DECEMBER 2025
PERTH OTOLOGY & TEMPORAL BONE COURSE
Perth, Australia 6-7 December asohns.org.au
Washington DC in November.
The British Academy of Audiology annual conference 2025 will be in Telford, Shropshire, England in November.
ASOHNS will run temporal bone surgical and dissection courses in Melbourne, Sydney and Perth.
Image:Vadim/stock.adobe.com.
Image: Martina/stock.adobe.com.
Service like no other
In a world often moving away from the human touch, Starkey remains steadfast in providing personalised points of interaction and always going that extra mile –all so we can serve you and your patients better than anyone else.
Excellence in Service
We strive to be the easiest company to do business with, and our partners have noticed. You can depend on them to take care of you.
When I phone Starkey, a human being is answering every single time.